
 Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Recognize signs and symptoms of anaphylaxis
- Define the grade and management of anaphylaxis
Definition and mechanisms
- Anaphylaxis is a severe and potentially life-threatening allergic reaction that develops suddenly and requires immediate medical attention
- The most common anaphylactic reactions are to foods, insect stings, medications, and latex
- Tissues in different parts of the body release histamine and other substances and this causes the airways to tighten
Signs and symptoms
- Sweating
- Rash/hives
- Nausea
- Vomiting or diarrhea
- Wheezing/shortness of breath due to airway constriction or swollen throat
- Fainting with loss of consciousness
- Angioedema
- Hypotension
- Tachycardia
Anaphylaxis grades
| Dermal | Abdominal | Respiratory | Cardiovascular | |
|---|---|---|---|---|
| Grade I | Erythema Urticaria Angioedema | |||
| Grade II | Erythema Urticaria Angioedema | Nausea Cramping | Bronchospasm | Moderate Hypotension Tachycardia |
| Grade III | Erythema Urticaria Angioedema | Nausea Vomiting Diarrhea | Severe Bronchospasm | Life-threatening Hypotension Tachycardia or bradycardia with or without Intraoperative arrhythmias |
| Grade IV | Erythema Urticaria Angioedema | Vomiting Defecation Diarrhea | Respiratory arrest | Peripartum cardiac arrest |
Management
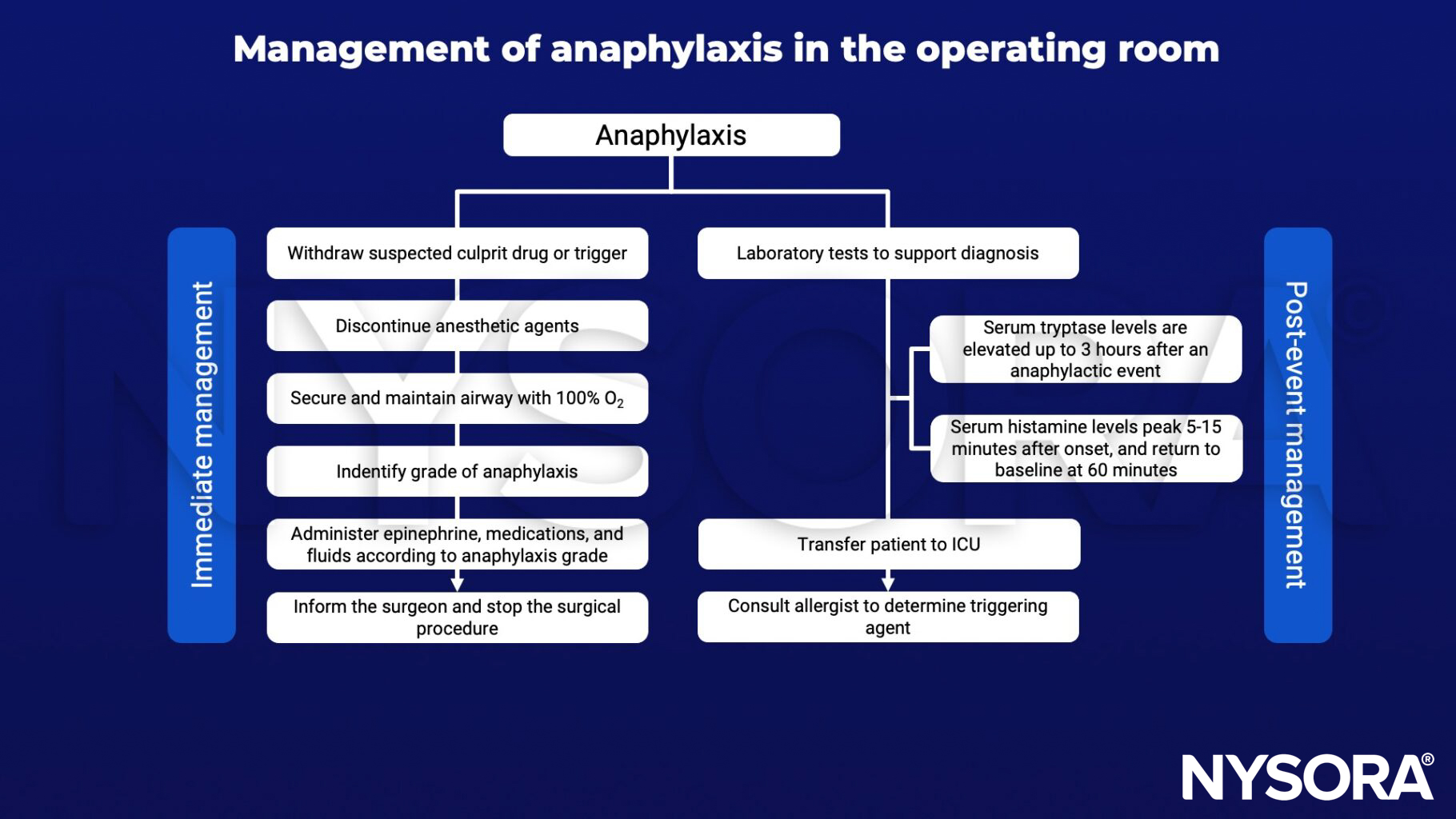
Treatment of anaphylaxis grades
| Intravenous epinephrine | Intravenous fluids (crystalloids) | |
|---|---|---|
| Grade II | Start with 20 μg bolus IV Inadequate response after 2 minutes: escalate to 50 μg and repeat every 2 minutes If no i.v. access: administer 300 μg i.m. | 500 ml rapid bolus Review response Repeat as needed |
| Grade III | 50 μg bolus or 100 μg bolus IV if inadequate response to other vasopressors or bronchodilators Inadequate response at 2 min: escalate to 200 μg and repeat every 2 minutes | 1L rapid bolus Review response Repeat as needed up to 30 ml kg-1 |
| Grade IV | 500 mcg IM/IV over 3 minutes followed by a continuous infusion (4-10 µg/min) Repeat as per ALS guidelines Suggest ECM if systolic <50 mmHg or endtidal CO2 <3 kPa (20 mmHg) | |
| Refractory anaphylaxis: inadequate response >10 min after symptom onset | Double epinephrine dose If response after more than three boluses of epinephrine IV is inadequate, add epinephrine infusion 0.05–0.1 μg/kg/min Hypotension - consider adding: Vasopressin 1–2 IU with or without infusion 2 IU/h Glucagon 1–2 mg (if on beta-adrenergic receptor blockers) Norepinephrine infusion 0.05–0.5 μg/kg/min Suggest ECLS: where available Bronchospasm - add: inhaled or i.v. bronchodilators (β2-agonist such as salbutamol or albuterol) |
Suggested reading
- Garvey LH, Dewachter P, Hepner DL, et al. Management of suspected immediate perioperative allergic reactions: an international overview and consensus recommendations. Br J Anaesth. 2019;123(1):e50-e64.
- Dewachter P, Mouton-Faivre C, Emala CW. Anaphylaxis and anesthesia: controversies and new insights. Anesthesiology. 2009;111(5):1141-1150.
Clinical updates
Savic et al. (Anesthesiology, 2025) provide an updated review of sugammadex-associated hypersensitivity, highlighting that although rare, sugammadex can trigger perioperative anaphylaxis and may involve both IgE-mediated and non–IgE pathways, such as direct mast cell activation or complement activation. The authors emphasize that reactions can occur even on first known exposure, discuss the diagnostic limitations of skin and in vitro testing, and emphasize that prompt recognition and treatment with epinephrine are critical. These findings underscore sugammadex as an important but uncommon cause of perioperative anaphylaxis, requiring vigilance, documentation, and structured allergy follow-up.











