Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Describe tracheoesophageal fistula and esophageal atresia, and their classification
- Define the associated congenital anomalies of tracheoesophageal fistulas
- Anesthetic management of pediatric patients with a tracheoesophageal fistula and/or esophageal atresia
Definition and mechanisms
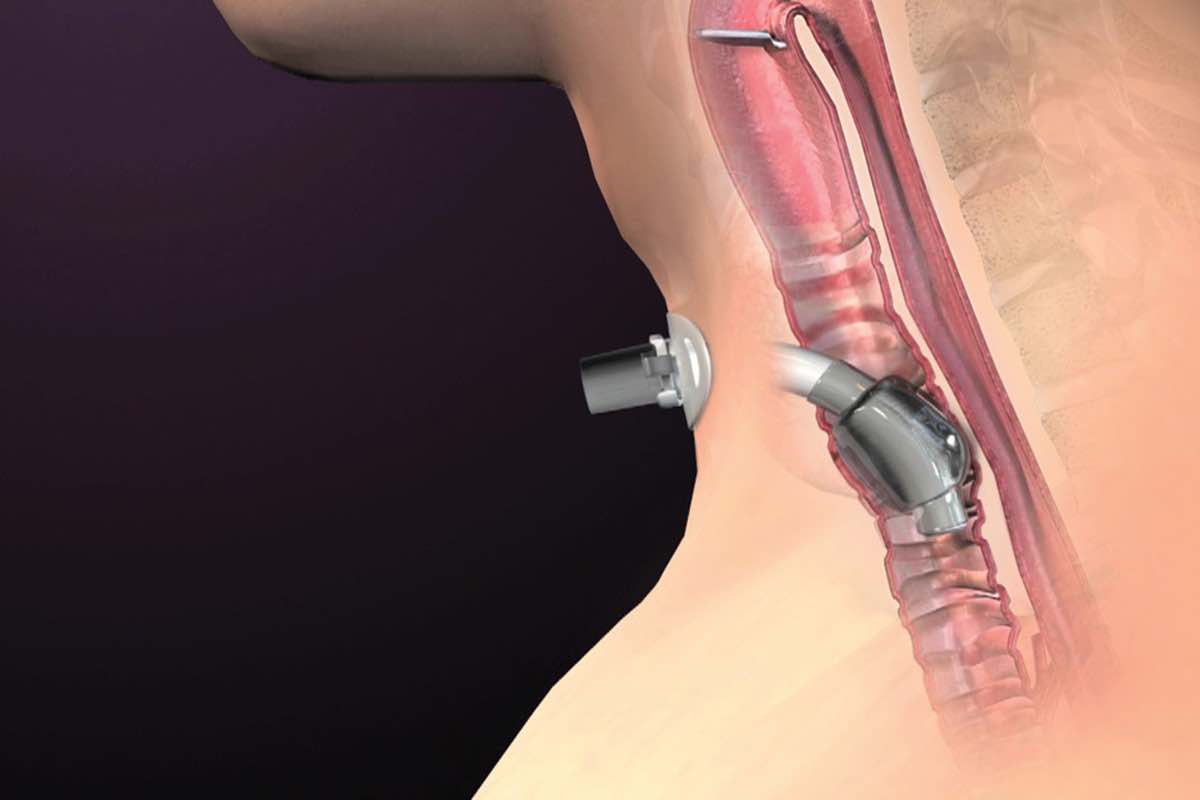
- A tracheoesophageal fistula (TEF) is one of the most common congenital anomalies and is an abnormal connection (fistula) between the esophagus and trachea
- TEF commonly occurs with esophageal atresia (EA), a related congenital malformation with a similar presentation to TEF
- EA is an abnormal connection between the esophagus and stomach, the esophagus ends in a blind-ended pouch rather than connecting normally to the stomach, can occur with or without the presence of a fistula
Classification
| Type A | No TEF, only EA → isolated EA The esophagus is divided into two parts with both portions ending in blind pouches | 8% of all cases |
| Type B | Proximal TEF and distal EA The lower portion of the esophagus ends in a blind pouch and the upper portion is connected to the trachea by a TEF | 2% of all cases |
| Type C | Proximal EA and distal TEF The upper portion of the esophagus ends in a blind pouch and the lower portion is connected to the trachea by a TEF | Most common, 85% of all cases |
| Type D | Both proximal and distal TEF TEF connects both the upper and lower portions of the esophagus and trachea | Rarest form, <1% of all cases |
| Type E (H-type) | Isolated TEF The esophagus connects to the stomach normally and is fully intact, a TEF connects the esophagus and trachea | 4% of all cases |
Signs and symptoms
- Excessive oral secretions, salvation
- Breathing difficulties, respiratory distress
- Coughing or choking when feeding
- Vomiting
- Cyanosis, especially during feeding
- Feeding difficulties
- Frequent lung infections
- Risk of aspiration
- EA and the inability to swallow may cause polyhydramnios in utero
Associated congenital anomalies
50% of babies with TEF/EA also have associated congenital anomalies
- Prematurity (30%)
- Congenital heart disease (30%): Ventricular septal defect, tetralogy of Fallot, patent ductus arteriosus, atrial septal defect, right-sided aortic arch
- Gastrointestinal anomalies (14%): Diaphragmatic hernia, duodenal atresia, pyloric stenosis, imperforate anus, malrotation, omphalocele
- Genitourinary anomalies (14%): Renal agenesis, hypospadias, horseshoe/polycystic kidney, ureteric/urethral abnormalities
- Musculoskeletal anomalies (10%): Radial limb abnormalities, polydactyly, lower limb defects, hemivertebrae, rib defects, scoliosis
- VACTERL syndromes (10%)
- Respiratory anomalies (6%): Tracheobronchomalacia, pulmonary hypoplasia, tracheal agenesis/stenosis, tracheal upper pouch
- Chromosome abnormalities (4%): Trisomy 13, 18, or Down syndrome
Treatment
- Surgical correction with resection of any fistula and anastomosis of any discontinuous segments
- Usually repaired within 24 hours of birth to minimize the risk and complications of aspiration
- Complications after surgery
- Anastomotic leaks
- Esophageal strictures (abnormal tightening)
- Damage to the laryngeal nerve
- Recurrence of the fistula
- Gastroesophageal reflux disease
- Dysphagia
- Asthma-like symptoms: Persistent coughing or wheezing
- Recurrent chest infections
- Tracheomalacia
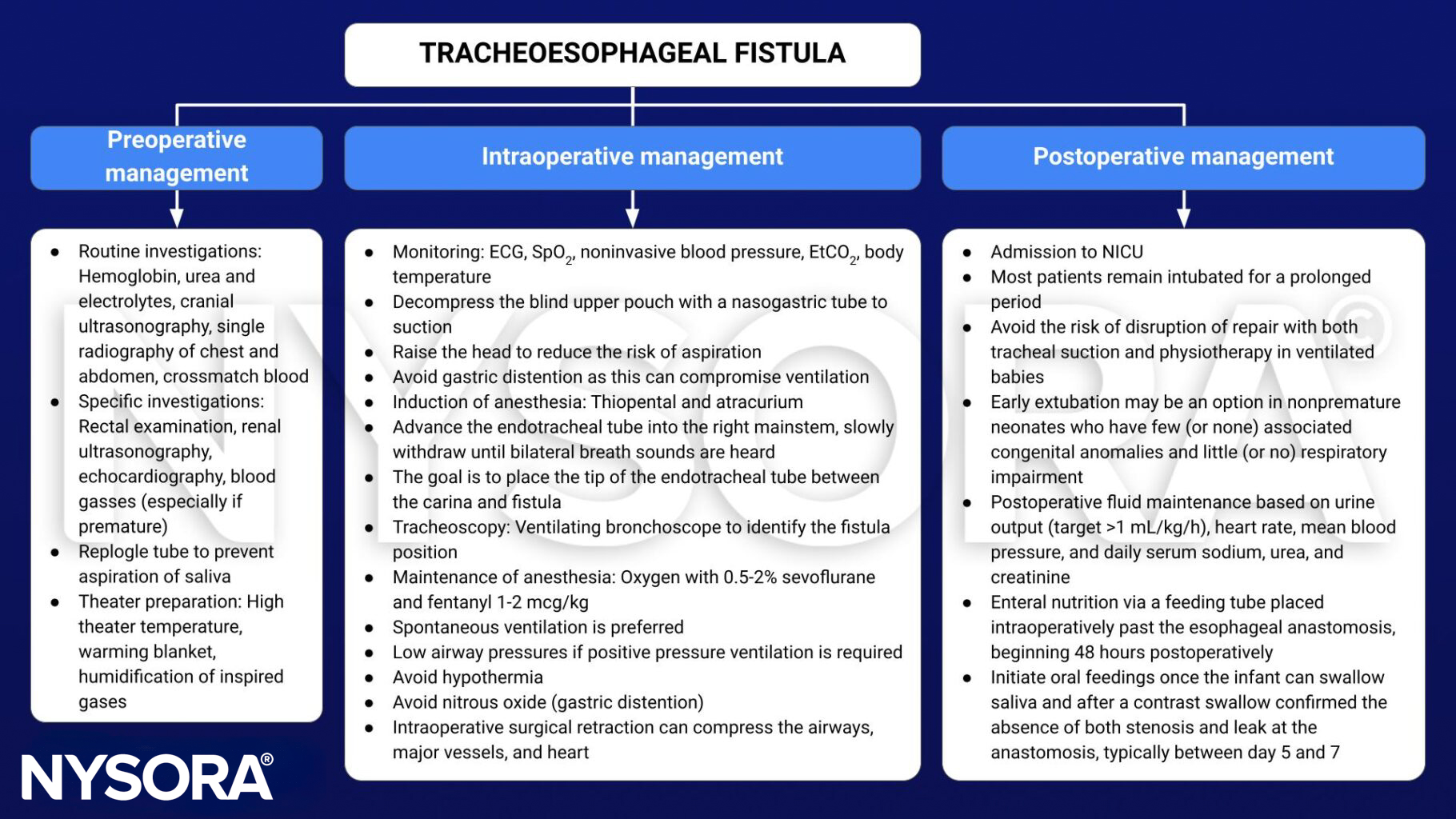
Management
Suggested reading
- Pollard BJ, Kitchen G. Handbook of Clinical Anaesthesia. 4th ed. Taylor & Francis group; 2018. Chapter 24 Paediatrics, Lomas B.
- Choumanovai I, Sanusii A, Evansii F. Anaesthetic management of tracheo-oesophageal fistula/ oesophageal atresia. WFSA. October 17, 2017. Accessed February 16, 2023. https://resources.wfsahq.org/atotw/anaesthetic-management-of-tracheo-oesophageal-fistula-oesophageal-atresia/
- Saraiya NR. TRACHEOESOPHAGEAL FISTULA. In: Houck PJ, Haché M, Sun LS. eds. Handbook of Pediatric Anesthesia. McGraw Hill; 2015. Accessed February 16, 2023. https://accessanesthesiology.mhmedical.com/content.aspx?bookid=1189§ionid=70363324