Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Describe the difference between omphalocele and gastroschisis
- Anesthetic management of pediatric patients with abdominal wall defects
Definition and mechanisms
- Omphalocele and gastroschisis are congenital abdominal wall defects resulting in intestinal herniation from the abdominal cavity
- Resulting from major defects in the closure of the abdominal wall → exposure of abdominal viscera
- Main difference: There is no sac covering the intestines in gastroschisis
- Both can be detected antenatally using fetal ultrasound → allows timing, location, and mode of delivery to be planned in advance
- Omphalocele: Deliver at term
- Gastroschisis: Benefit from early delivery (37 weeks gestation) to limit bowel damage from exposure to amniotic fluid
- Both are associated with prematurity and low birth weight
Omphalocele
- Herniation of abdominal contents through the middle of the abdominal wall at the umbilicus
- The skin, muscle, and fibrous tissue are missing
- The intestines herniate through the opening and are covered by a thin sac
- The sac is formed from an outpouching of the peritoneum and protrudes in the midline, through the umbilicus
- Commonly occurs with other congenital defects (e.g., heart and kidney defects), chromosome abnormalities (e.g., Down syndrome, trisomy 18, trisomy 13), and genetic syndromes (e.g., Beckwith-Wiedemann syndrome)
Gastroschisis
- Herniation of abdominal contents from a defect lateral to the umbilicus (usually right-sided), but not directly over it
- Protruding organs are not covered by a thin sac → damage due to direct contact with amniotic fluid in the uterus → inflammation
- Rarely have other congenital defects, seldom associated with chromosome abnormalities or genetic syndromes
Signs and symptoms
- External herniation of abdominal viscera
Omphalocele
- Omphalocele minor: Minor herniation into the umbilical cord, small 5-8 cm defect
- Omphalocele major: Large defect, including the liver, with poorly developed abdominal and pulmonary hypoplasia
- Intestine looks normal
Gastroschisis
- The intestine wall may be thickened, with a fibrin “peel” due to exposure to amniotic fluid
- May involve the stomach, bladder, uterus, and rarely liver
Complications
- Intrauterine growth retardation
- Underdevelopment of the lungs → respiratory insufficiency may require mechanical ventilation
- Feeding difficulties
- Poor gut motility
- Malrotation
- Intestinal atresia
- Volvulus
- Stenosis
- Gastroesophageal reflux
- Short bowel syndrome → dehydration
Sequelae of an open abdomen
- Aspiration
- Hypothermia
- Fluid and electrolyte abnormalities
- Sepsis
Treatment
Initial post-delivery treatment
- Fluid resuscitation
- Care of herniated bowel/viscera and their blood supply: Cover exposed organs with a sterile dressing to keep them moist and protected
- Bowel decompression using a nasogastric tube
- Temperature regulation: Nurse in an incubator to reduce heat loss
- Omphalocele: Inspect the sac to check whether or not it is ruptured
- IV antibiotics to minimize the risk of infection
Single vs staged surgery
- Surgery typically takes place shortly after birth
- Omphalocele: Semi-urgent surgery unless sac is ruptured
- Gastroschisis: Urgent surgery
- Required to replace the intestines in the abdomen and to close the opening
- Single stage surgery: Omphalocele minor
- Intestines are moved back in the abdomen, and the opening is closed during the same surgery
- Staged surgery: Omphalocele major and gastroschisis
- Wrap intestines in a protective covering (i.e., silo)
- Gradually move intestines back into the abdomen over several days or weeks
- Surgically close the opening once all intestines are back in the abdomen
Management
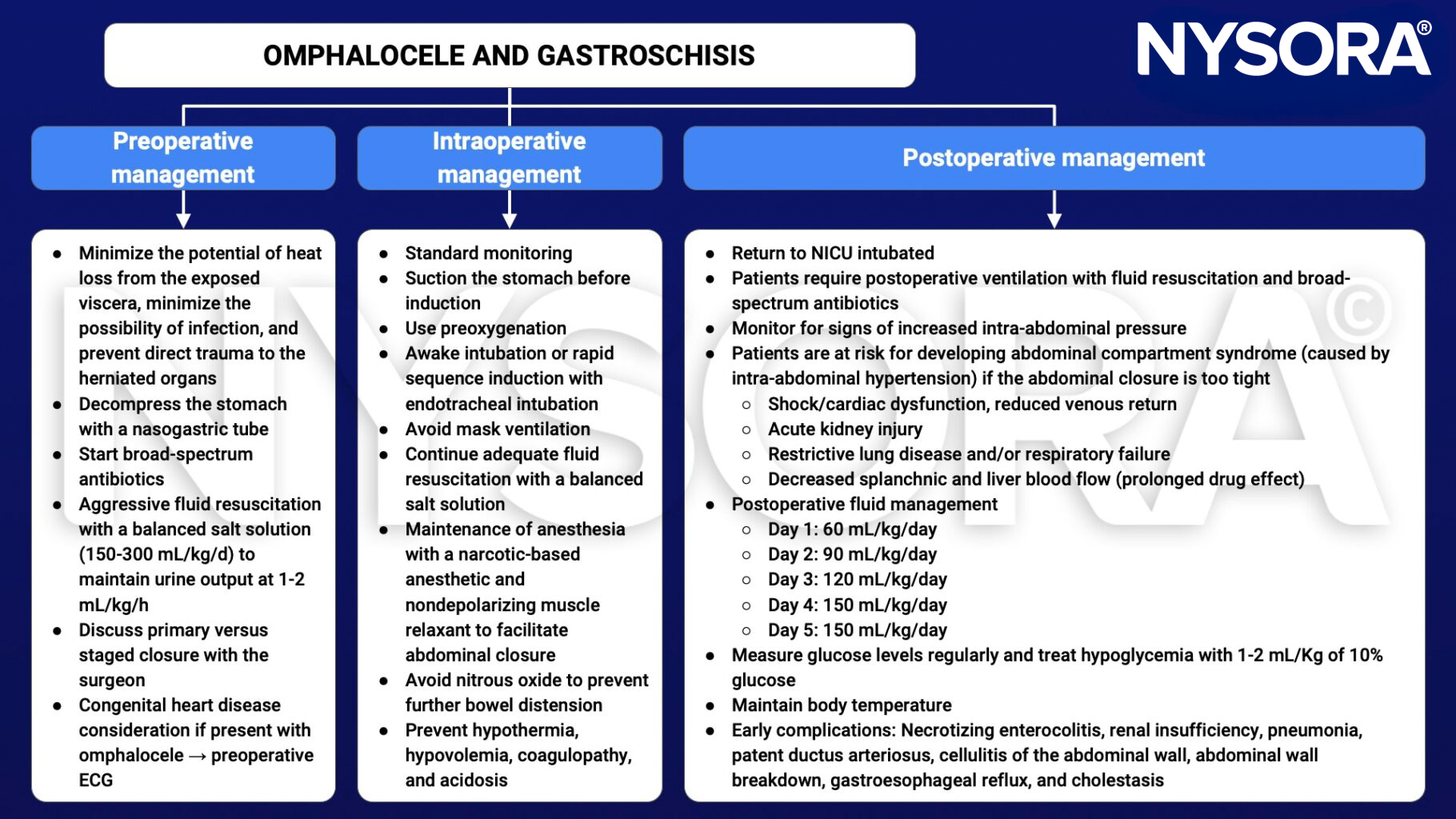
Keep in mind
- Neonates are highly susceptible to dehydration and heat loss before repair of the abdominal wall defect → fluid resuscitation and temperature control
- Repair surgery may be primary or staged
- Improved survival is associated with optimal pre- and postoperative care
Suggested reading
- Saraiya NR. GASTROSCHISIS AND OMPHALOCELE. In: Houck PJ, Haché M, Sun LS. eds. Handbook of Pediatric Anesthesia. McGraw Hill; 2015. Accessed February 14, 2023. https://accessanesthesiology.mhmedical.com/content.aspx?bookid=1189§ionid=70363342
- Poddar R, Hartley L. Exomphalos and gastroschisis. Continuing Education in Anaesthesia Critical Care & Pain. 2009;9(2):48-51.
- Wouters K, Walker I. Neonatal anaesthesia 2: Anaesthesia for neonates with abdominal wall defects. WFSA. August 28, 2008. Accessed February 14, 2023. https://resources.wfsahq.org/atotw/neonatal-anaesthesia-2-anaesthesia-for-neonates-with-abdominal-wall-defects/