Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Describe the indications for esophagectomy
- Manage patients presenting for esophagectomy
Background
- Esophageal cancer is the eighth most common malignancy worldwide
- Curative therapy for many patients involves surgery (esophagectomy), often with preoperative chemotherapy
- Esophagectomy remains high-risk with substantial associated morbidity and mortality
Risk factors for esophageal malignancy
| Risk factor | Adenocarcinoma | Squamous cell carcinoma |
|---|---|---|
| Lifestyle | Smoking | Alcohol, smoking (may show synergism), poor oral hygiene |
| Racial origin | Caucasian more common than Asian or African | Sub-Saharan African Heritage three times higher than Caucasians |
| Far East Asian Heritage | ||
| Age and gender | Increasing age, male greater than female | Male greater than female |
| Dietary | Low dietary intake of fruit and vegetables | Salted vegetables, preserved fish |
| Disease | Gastro-oesophageal reflux, Barrett’s oesophagus, obesity, family history (rare) | Mutations of alcohol metabolic pathways, achalasia, caustic injury, nutritional deficiencies, non-epidermolytic palmoplantar keratoderma |
| Economic | Developed world | Low socioeconomic status |
| Developing world | ||
| Medical/industrial | Thoracic radiation, medications that relax the lower oesophageal sphincter | Thoracic radiation |
Risk factors for perioperative morbidity and mortality
- Poor cardiac and/or pulmonary function
- Advanced age
- Tumor stage
- Diabetes mellitus
- Impaired general health
- Hepatic dysfunction
- Peripheral vascular disease
- Smoker
- Chronic use of steroids
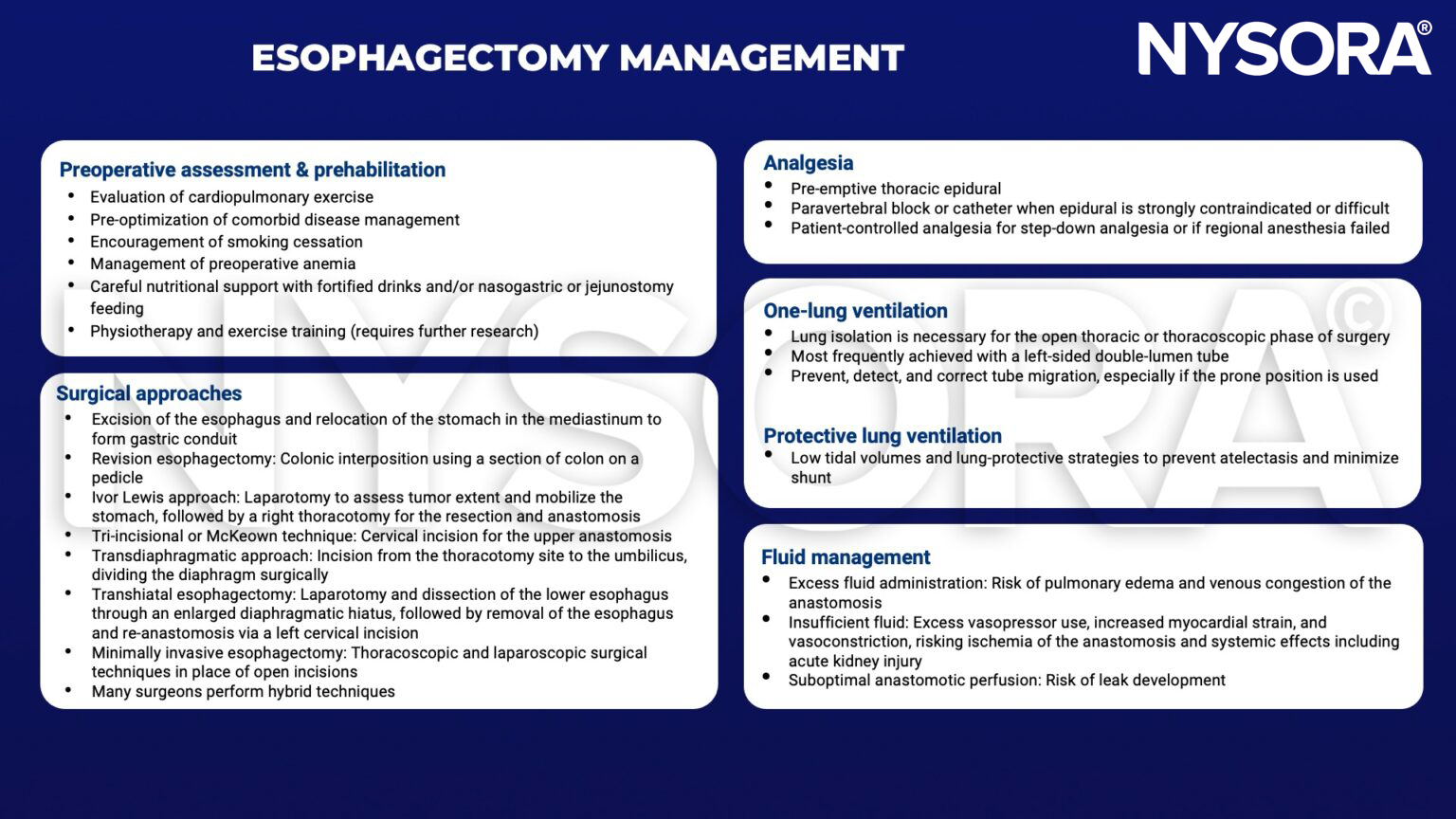
Management
Postoperative complications
| Respiratory | Pneumonia |
| Atelectasis | |
| Acute respiratory stress syndrome | |
| Recurrent laryngeal nerve palsy | |
| Surgical | Anastomotic leak |
| Cardiac | Supraventricular arrhythmias (e.g., atrial fibrillation) |
- The risk of respiratory complications can be minimized by adequate analgesia, reversal of muscular block, normothermia, chest physiotherapy and hemodynamic stability
- Major anastomotic leaks require surgical exploration and revision surgery
- Smaller leaks are managed by keeping the patient nil by mouth, giving high protein enteral feed or total parenteral nutrition, antibiotics, chest physiotherapy, radiologically guided drainage collection and performing serial contrast studies
Suggested reading
- Howells P, Bieker M, Yeung J. Oesophageal cancer and the anaesthetist. BJA Education. 2017;17(2):68-73.
- Veelo DP, Geerts BF. Anaesthesia during oesophagectomy. J Thorac Dis. 2017;9(Suppl 8):S705-S712. doi:10.21037/jtd.2017.03.153
Clinical Updates
Hovgaard et al. (Anesthesiology, 2026) report that in 100 esophagectomy patients, an individualized perioperative hemodynamic strategy using patient-specific nighttime MAP targets and extended goal-directed fluid therapy through the first postoperative morning did not reduce 30-day overall morbidity versus standard care. The intervention achieved higher MAPs and required more crystalloids, greater total fluid balance, and substantially more norepinephrine, but without improvements in 90-day complications, ICU stay, or total hospital stay, suggesting that extending individualized blood pressure and flow optimization after esophagectomy does not translate into better clinical outcomes.
- Read more about this HERE.