
 Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Describe congenital diaphragmatic hernia
- Understand the predictors for survival in congenital diaphragmatic hernia
- Management of congenital diaphragmatic hernia
Definition and mechanisms
- Congenital diaphragmatic hernia (CDH) is a birth defect characterized by the development of a hole in the diaphragm, leading to the protrusion of abdominal contents into the thoracic cavity affecting the normal development of the lungs
- 90% is left-sided
- Infants born with CDH experience respiratory failure due to pulmonary hypertension and pulmonary hypoplasia (decreased lung volume)
- Newborns born with CDH require immediate care at delivery → delivery should be as close to term as possible
- CDH is a life-threatening condition → death occurs due to
- Inadequate gas exchange surface
- Fixed high pulmonary vascular resistance (decreased vascular cross-sectional area, normal cardiac output)
- Reversible pulmonary hypertension
- Pneumothorax
- Additional anomalies (5%) and complications of intensive therapy
Diagnosis and survival
- CDH is usually discovered during a routine prenatal ultrasound
- The stomach, intestines, or liver may be present in the fetus’ chest where the lungs should be; the fetus’ heart may also be pushed to one side by the extra organs in the chest
Antenatal ultrasound predictors of survival in CDH
- Calculate the lung-to-head ratio (LHR) by dividing the fetal lung area (mm2) by the fetal head circumference (mm)
- LHR >1.35: 100% survival
- LHR 1.35 to 0.6: 61% survival
- LHR <0.6: No survival
- Calculate the observed to expected LHR (O/E LHR) by dividing the observed LHR by the expected ratio for gestational age
- The fetal lung area increases 16-fold compared to a 4-fold increase in the head circumference between 12 and 32 weeks of gestation
- O/E LHR <25%: Severe CDH (survival 10% with liver up and 25% with liver down)
- O/E LHR <15% with liver up: No survival
- Position of the liver (or presence of liver herniation)
- Liver herniation with LHR <1.0: 60% mortality
- Liver in the thorax: 56% survival
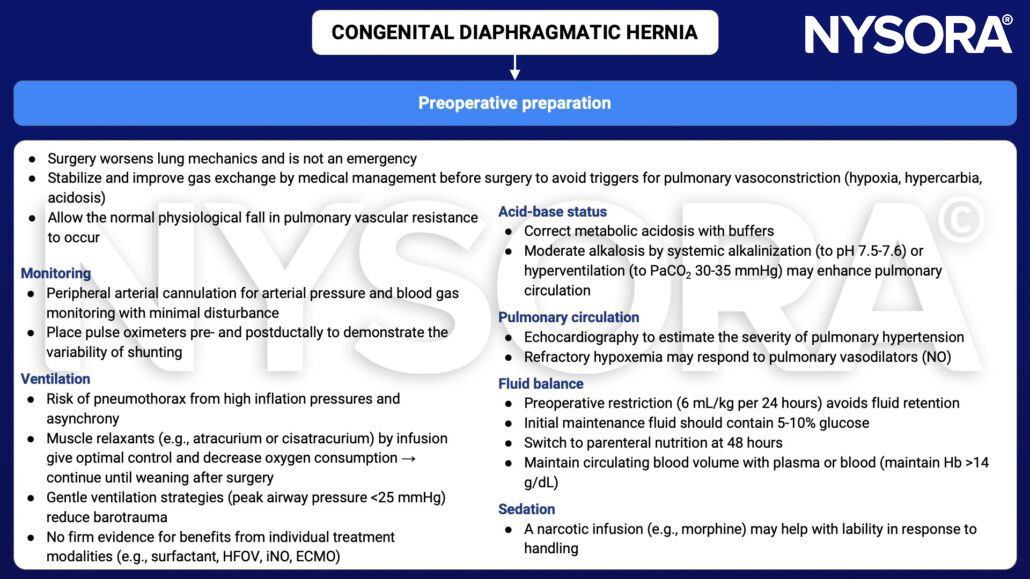
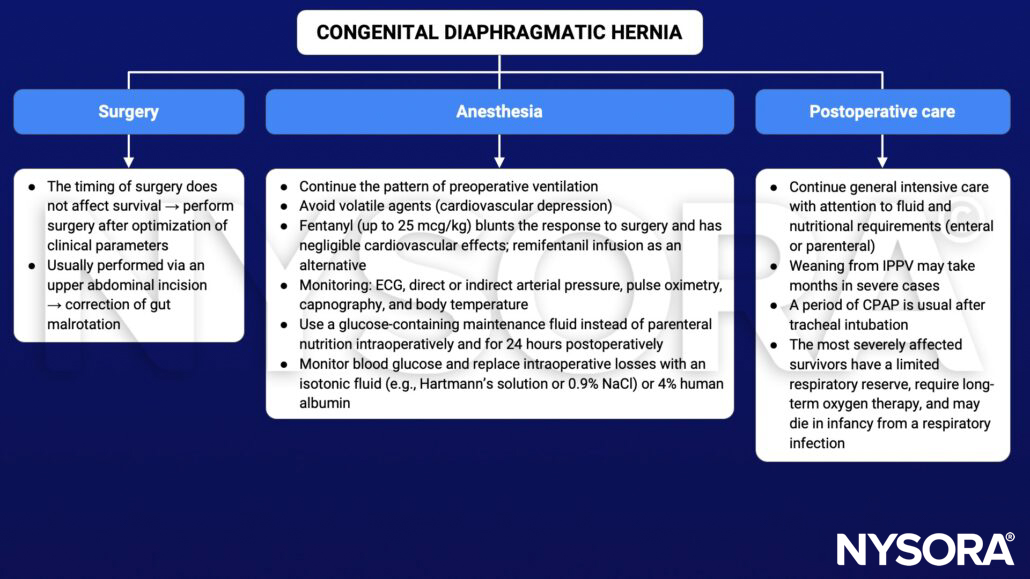
Anesthetic considerations
- Emergency situation
- Critically ill neonate
- Hypoplastic lungs
- Respiratory insufficiency (hypoxemia, hypercarbia, acidosis)
- Permissive hypercarbia may be required
- Consider HVO or ECMO
- Pulmonary hypertension
- Potential for right ventricle failure, reduced cardiac output
- Consider inhaled NO
- Transitional circulation
- Potential for right-left and left-right shunting
- Patent ductus arteriosus
- Delayed surgical repair, resuscitation is first priority
- NICU required
Management
Resuscitation
- Call NICU
- Indication for immediate tracheal intubation to facilitate intermittent positive pressure ventilation (IPPV)
- No bag-mask ventilation → distends herniated viscera, worsens mediastinal shift, and increases the risk of pneumothorax; while barotrauma further damages the hypoplastic lungs
- Nasal intubation helps with fixation and ventilator compliance
- Pass a nasogastric tube to deflate the gut and keep on free drainage
- Umbilical artery/vein lines
- ABG, chest X-ray, echocardiogram
- Lung protective ventilation
- Target SaO2 >85% and permissive hypercapnia (PaCO2 <65 mmHg, pH >7.25)
- PCV or PSV PIP <25 cmH2O
- Inspiratory time 0.35 sec
- PEEP 3-5 mmHg
- RR <65
- Consider HVO, iNO, or ECMO
- Consider NO and inotropes for pulmonary hypertension
- Fluid: Target MAP 45-50 mmHg
- Sedation: Opioids and benzodiazepines, thoracic epidural
- Avoid neuromuscular blocking drugs
Keep in mind
- Immediate management at birth includes bowel decompression, avoidance of mask ventilation, and endotracheal tube placement if required
- The main focus of management includes gentle ventilation, hemodynamic monitoring, and treatment of pulmonary hypertension, followed by surgery
Suggested reading
- Leininger K, Chiu K. Anesthetic Considerations In Congenital Diaphragmatic Hernia. [Updated 2022 Nov 15]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan. Available from: https://www.ncbi.nlm.nih.gov/books/NBK572077/
- Pollard BJ, Kitchen G. Handbook of Clinical Anaesthesia. 4th ed. Taylor & Francis group; 2018. Chapter 24 Paediatrics, Lomas B.
- Chandrasekharan PK, Rawat M, Madappa R, Rothstein DH, Lakshminrusimha S. Congenital Diaphragmatic hernia – a review. Matern Health Neonatol Perinatol. 2017;3:6.











