Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Describe the electrolyte and acid-base abnormalities associated with pyloric stenosis
- Explain why these electrolyte and acid-base abnormalities need to be corrected preoperatively
- Anesthetic management of a pediatric patient with pyloric stenosis
Definition and mechanisms
- Pyloric stenosis, or infantile hypertrophic pyloric stenosis, is an uncommon condition in infants characterized by abnormal thickening of the pylorus muscles in the stomach, leading to gastric outlet obstruction
- Typically seen between 2 and 12 weeks of age, patients present with projectile vomiting after feedings, dehydration, and failure to thrive
- The danger of pyloric stenosis comes from the dehydration and electrolyte disturbance rather than the underlying problem itself → infant has to be stabilized by correcting the dehydration and hypochloremic alkalosis with IV fluids
Signs and symptoms
- Symptoms usually appear within 3-5 weeks after birth
- Bile-free projectile vomiting after every feeding
- Persistent hunger
- Stomach contractions (visible peristalsis in the left upper quadrant from left to right)
- Changes in bowel movements
- Weight problems
Complications
- Failure to grow and develop, failure to thrive
- Dehydration, hypovolemia
- Metabolic alkalosis
- Electrolyte abnormalities (hypochloremia, hyponatremia, hypokalemia)
- Stomach irritation
- Jaundice
Risk factors
- First-born male children
- Preterm birth
- Cesarean section
- Family history
- Smoking during pregnancy
- Bottle feeding
- Early antibiotic use (e.g., erythromycin to treat whooping cough)
- White and Hispanic children
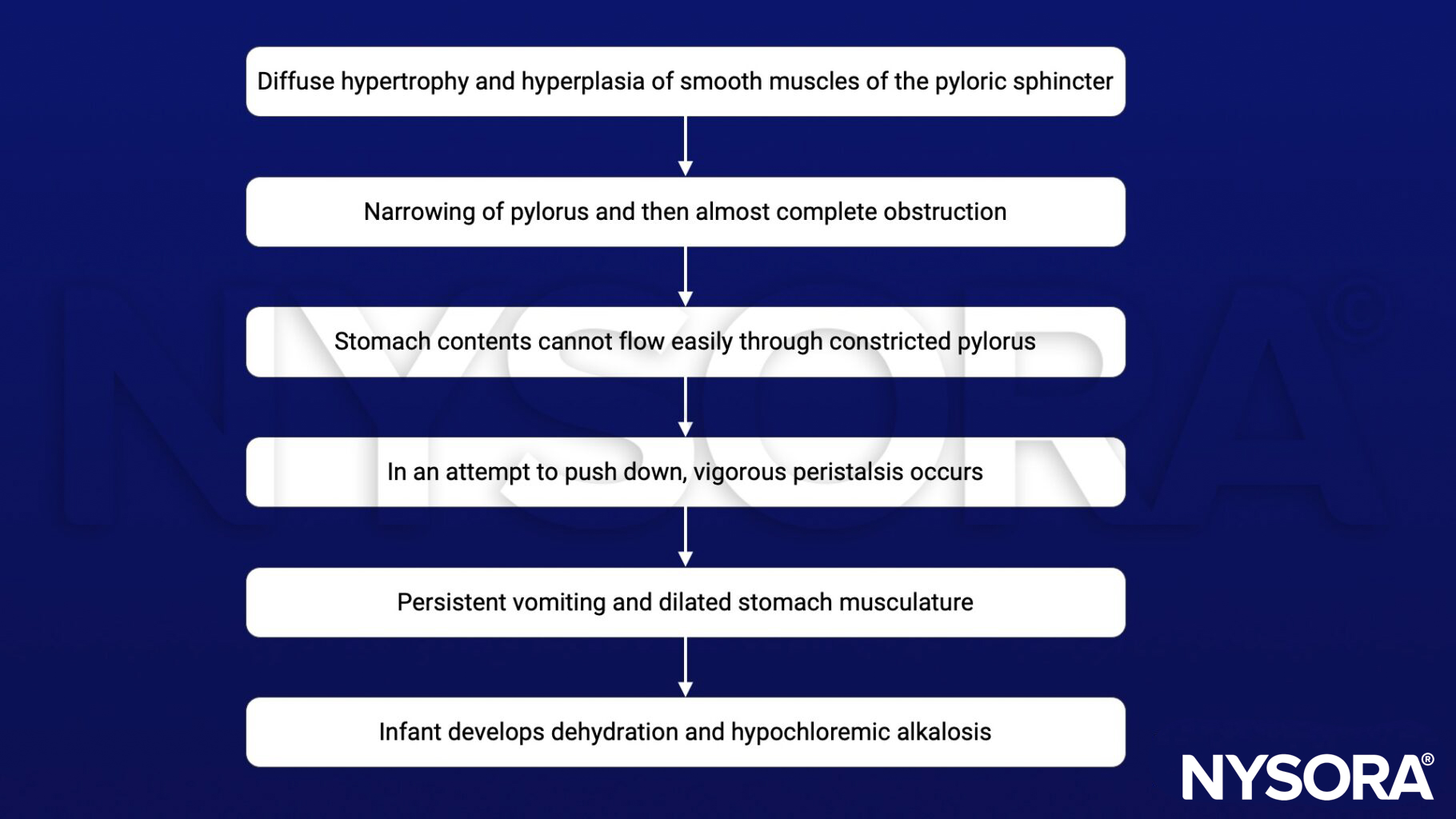
Pathophysiology
Treatment
- Correction of dehydration and hypochloremic alkalosis before surgery with IV fluids → accomplished within 24-48 hours
- Surgery: Pyloromyotomy
Management
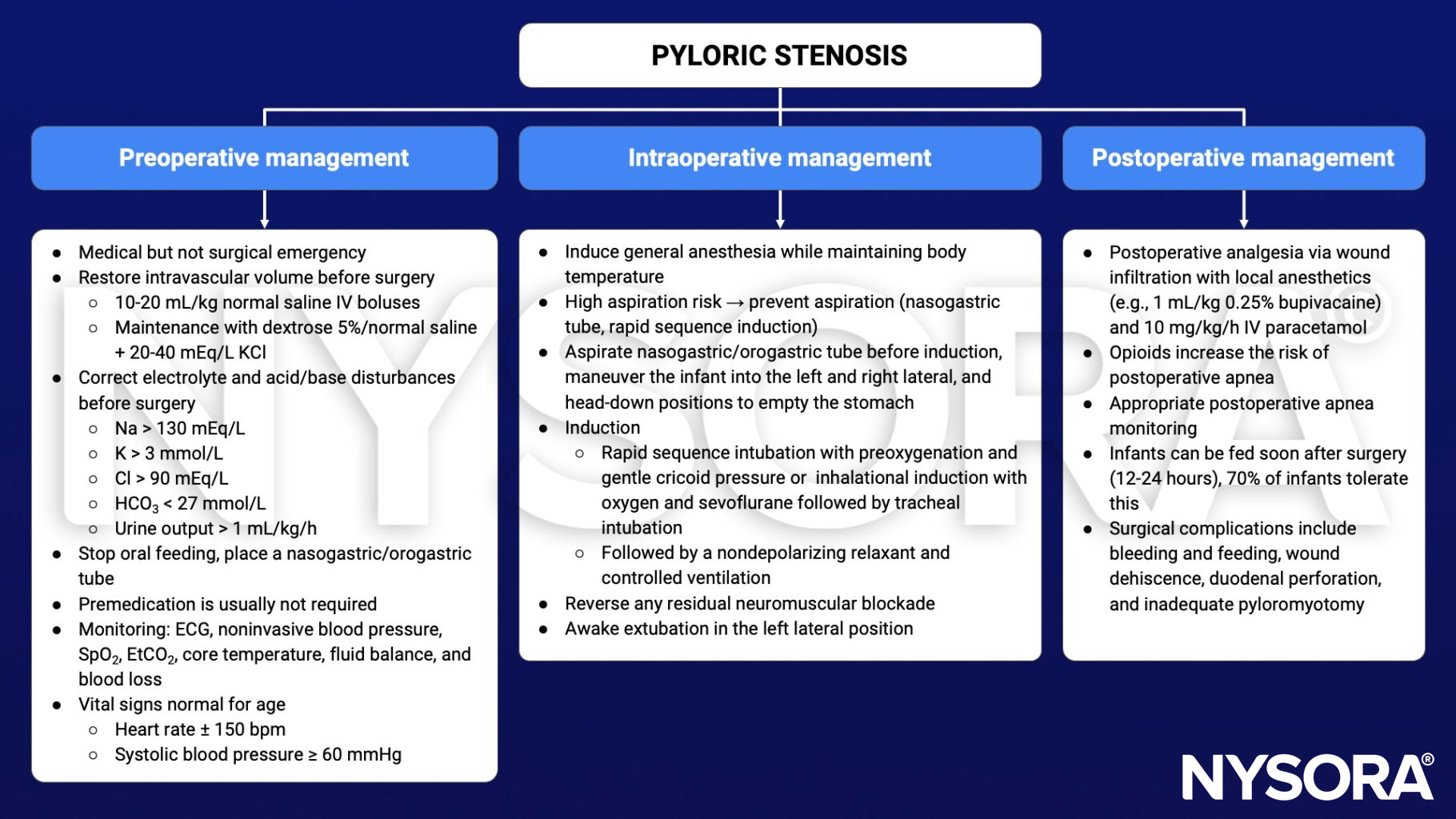
Keep in mind
- Vomiting associated with pyloric stenosis results in hypochloremia, hyponatremia, hypokalemia, metabolic alkalosis, and dehydration, all of which have to be corrected before general anesthesia and surgery
- Empty the stomach using a nasogastric or orogastric tube before induction of anesthesia
- Ensure an adequate depth of anesthesia with a complete neuromuscular block before laryngoscopy to minimize the risk of regurgitation and pulmonary aspiration
Suggested reading
- Craig R, Deeley A. Anaesthesia for pyloromyotomy. BJA Educ. 2018;18(6):173-177.
- Pollard BJ, Kitchen G. Handbook of Clinical Anaesthesia. 4th ed. Taylor & Francis group; 2018. Chapter 24 Paediatrics, Lomas B.
- Houck PJ. PYLORIC STENOSIS. In: Houck PJ, Haché M, Sun LS. eds. Handbook of Pediatric Anesthesia. McGraw Hill; 2015. Accessed February 14, 2023. https://accessanesthesiology.mhmedical.com/content.aspx?bookid=1189§ionid=70363285