
 Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Describe rheumatoid arthritis
- Recognize the symptoms and signs of rheumatoid arthritis
- Anesthetic management of a patient with rheumatoid arthritis
Definition and mechanisms
- Rheumatoid arthritis (RA) is a chronic autoimmune inflammatory disorder that mainly affects the synovial joints → symmetrical erosive polyarthropathy
- Early RA affects the smaller joints first (hands and feet)
- As RA progresses, symptoms spread to the wrists, knees, ankles, elbows, hips, and shoulders
- Periods of increased disease activity (flares) alternate with periods of relative remission
- RA also affects other organs in more than 15-25% of the cases → systemic
Signs and symptoms
- Tender, warm, swollen joints
- Joint stiffness that is usually worse in the mornings and after inactivity
- Fatigue, fever, loss of appetite
- The painful swelling can eventually result in bone erosion and joint deformity
Risk factors
- Female gender
- Family history
- Increasing age
- Smoking
- Overweight
Complications
- Osteoporosis
- Rheumatoid nodules
- Dry eyes and mouth (Sjogren’s syndrome)
- Infections
- Abnormal body composition
- Carpal tunnel syndrome
- Cardiovascular disease
- Lung disease
- Lymphoma
Extra-articular manifestations
- Neurological: Central neuropathy, peripheral neuropathy (carpal tunnel syndrome), autonomic neuropathy
- Ocular: Kerato-conjuctivitis
- Cardiovascular: Pericarditis, pericardial effusion, cardiac tamponade, valvular heart disease (usually regurgitation), conduction abnormalities, granulomatous disease, endocarditis or myocarditis, coronary artery disease
- Respiratory: Reduced chest wall compliance (costochondral disease), pleural effusion, restrictive lung disease, pulmonary nodule
- Hematological: Anemia [chronic disease, iron deficiency (bleeding) and bone marrow suppression from medication], thrombocytopenia, Felty’s syndrome, lymphoma
- Hepatic: Hepatic fibrosis, hepatomegaly with splenomegaly, hypoalbuminemia
- Renal: Glomerulonephritis, tubulointerstitial nephritis, amyloidosis
- Skin: Fragile skin, pyoderma gangrenosum, Sicca syndrome, scleritis, scleromalacia perforans
- Musculoskeletal: Osteoporosis
Treatment
- Medications: Relieve pain, reduce inflammation, slow down the progression of RA
- Non-steroidal anti-inflammatory drugs (NSAIDs): Ibuprofen and naproxen
- Corticosteroids: Prednisone
- Conventional disease-modifying anti-rheumatic drugs (DMARDs): Methotrexate, leflunomide, hydroxychloroquine, and sulfasalazine
- Biological DMARDs: Abatacept, adalimumab, anakinra, certolizumab, etanercept, golimumab, infliximab, rituximab, sarilumab, and tocilizumab
- Targeted synthetic DMARDs: Baricitinib, tofacitinib, and upadacitinib
- Physical therapy: To reduce pain and stiffness
- Surgery: Repair damaged joints to restore function and reduce pain
-
- Synovectomy
- Tendon repair
- Joint fusion
- Total joint replacement
Management
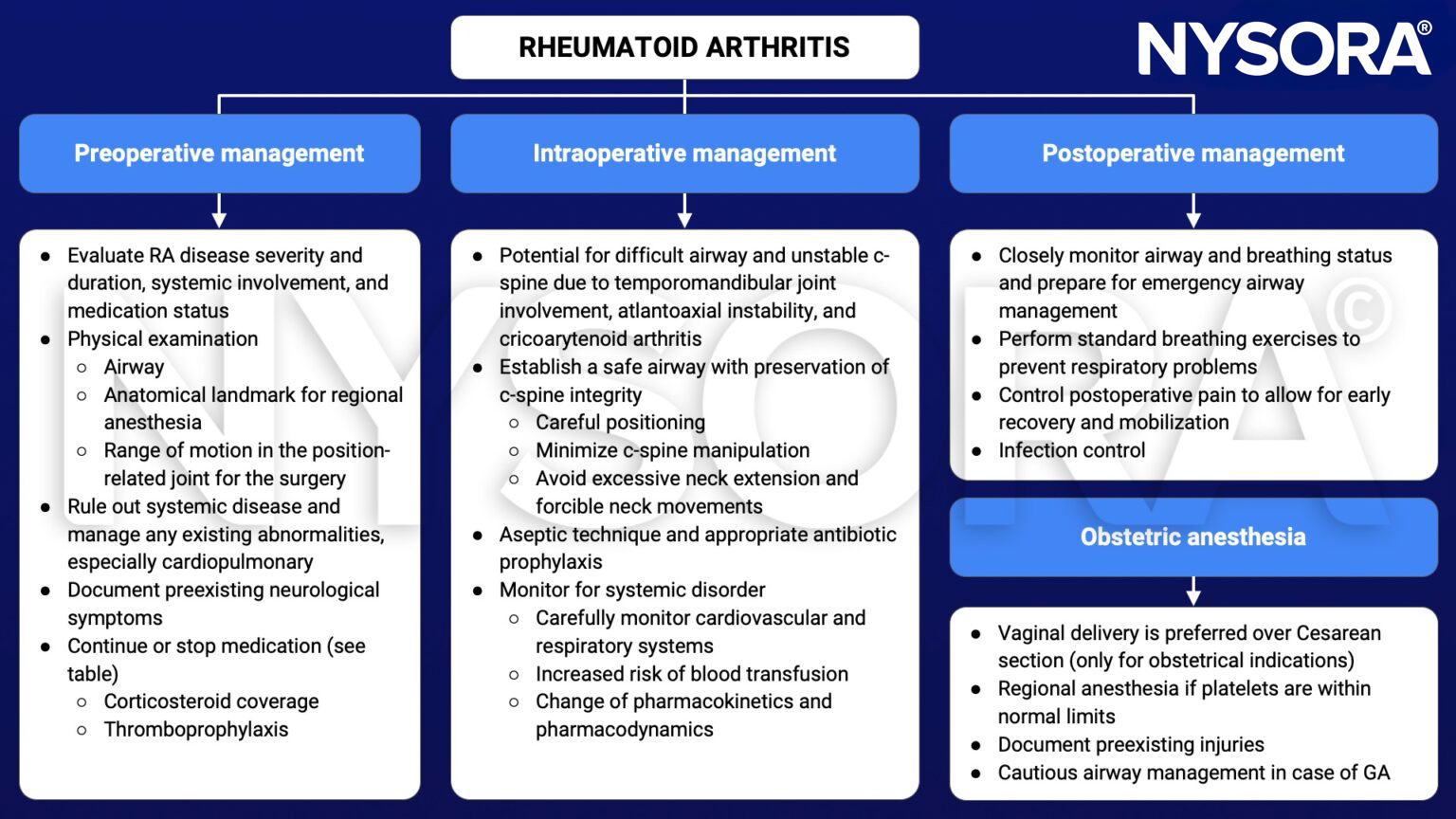
Recommendations on how to deal with RA medications during elective surgical procedures
| Medication | Administration during surgical procedure |
|---|---|
| Corticosteroids | See next table |
| Conventional DMARDs | Continue |
| Biologic DMARDs | Withhold before surgery and schedule surgery at the end of the dosing cycle |
| Targeted synthetic DMARDs | Withhold at least 7 days prior to surgery |
Recommended steroid doses during surgery
| Type of surgery | Endogenous cortisol secretion rate | Examples | Recommended steroid dosing |
|---|---|---|---|
| Superficial | 8-10 mg/day (baseline) | Dental surgery, biopsy | Usual daily dose |
| Minor | 50 mg/day | Inguinal hernia, colonoscopy, uterine curettage, hand surgery | Usual daily dose plus hydrocortisone 50 mg i.v. before incision + hydrocortisone 25 mg i.v. every 8 hrs for 1 day + usual daily dose |
| Moderate | 75-150 mg/day | Low extremity revascularization, total joint replacement, cholecystectomy, colon cancer, abdominal hysterectomy | Usual daily dose plus hydrocortisone 50 mg i.v. before incision + hydrocortisone 25 mg i.v. every 8 hrs for 1 day + usual daily dose |
| Major | 75-150 mg/day | Esophagectomy, total proctocolectomy, major cardiac/vascular surgery, hepaticojejenostomy, delivery, trauma | Usual daily dose plus hydrocortisone 100 mg i.v. before incision + continuous i.v. infusion of hydrocortisone 200 mg for >1 day or hydrocortisone 50 mg i.v. every 8 hours/day + taper dose by half/day until usual daily dose reached and continuous i.v. fluids with 5% dextrose and 0.2-0.45% sodium chloride, based on degree of hypoglycemia |
Keep in mind
- Carefully perform a preoperative evaluation to prevent complications and minimize injury
- Anesthetic management strategies should consider RA-related systemic problems
- Individualize postoperative management
Suggested reading
- Kim HR, Kim SH. Perioperative and anesthetic management of patients with rheumatoid arthritis. Korean J Intern Med. 2022;37(4):732-739.
- Samanta R, Shoukrey K, Griffiths R. Rheumatoid arthritis and anaesthesia. Anaesthesia. 2011;66(12):1146-1159.











