
 Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Describe Sjogren’s syndrome
- Recognize the symptoms and signs of Sjogren’s syndrome
- Anesthetic management of a patient with Sjogren’s syndrome
Definition and mechanisms
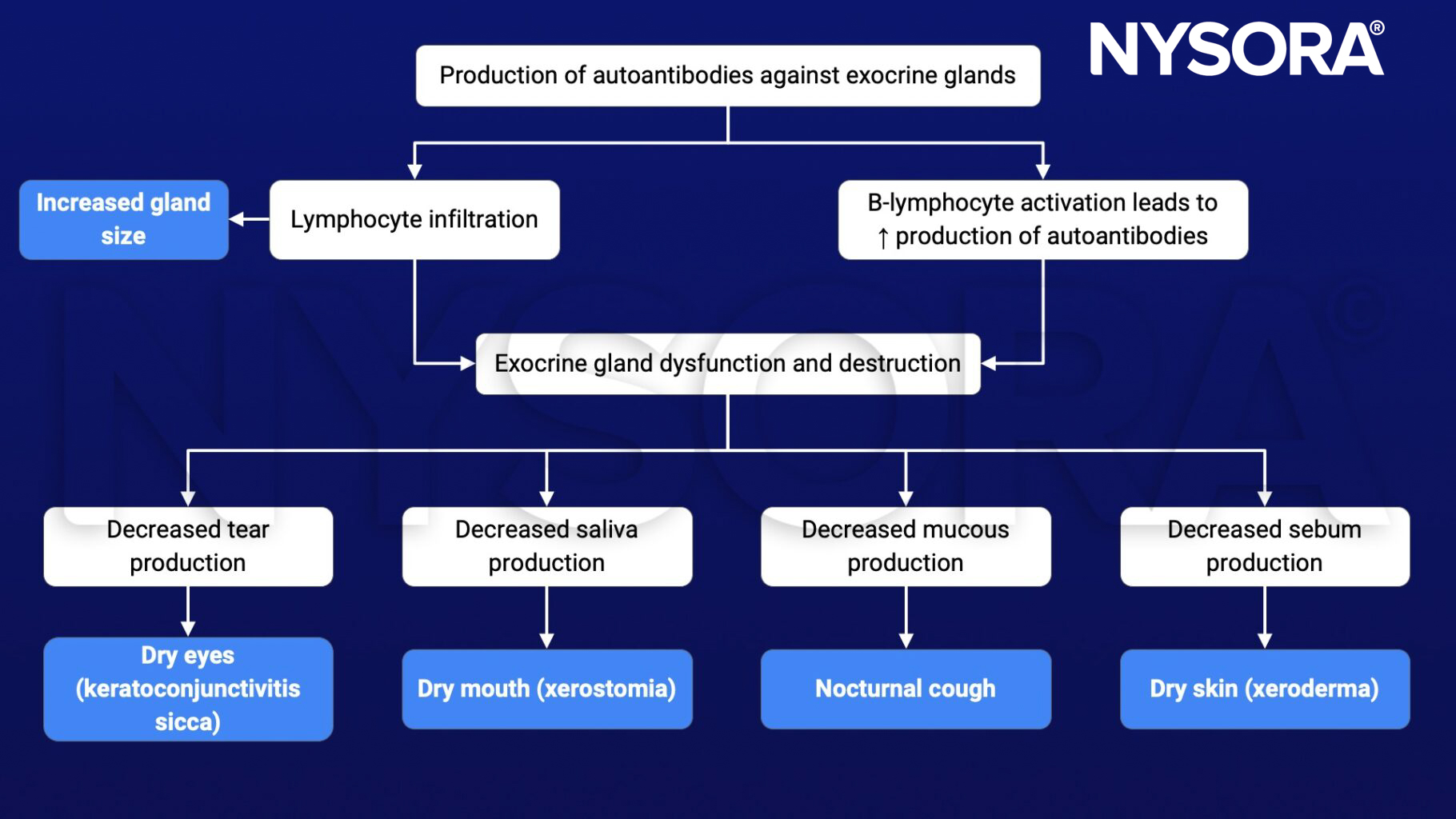
- Sjogren’s syndrome is a frequent autoimmune disease (autosomal recessive disorder) characterized by dysfunction and destruction of exocrine glands (e.g., lacrimal and salivary glands), associated with lymphocytes infiltrates and immunological hyperreactivity
- The hallmark symptoms of Sjogren’s syndrome are dry eyes and a dry mouth
- The condition often accompanies other immune system disorders (e.g., rheumatoid arthritis, systemic lupus erythematosus, and multiple sclerosis)
Signs and symptoms
- Dry eyes (keratoconjunctivitis sicca)
- Dry mouth (xerostomia)
- Joint pain, swelling, and stiffness
- Swollen salivary glands
- Skin rashes or dry skin (xeroderma)
- Vaginal dryness
- Chronic dry cough
- Prolonged fatigue
- Thyroid problems
Causes
- Genetic factors: Mutations in HLA-DR and HLA-DQ genes
- Environmental factors: Viruses (e.g., Epstein-Barr virus, hepatitis C, and human T-cell leukemia virus type 1), hormones (e.g., estrogen, prolactin), etc.
Complications
- Dental cavities
- Yeast infections
- Vision problems: Light sensitivity, blurred vision, and corneal damage
- Lymphoma
- Inflammation can cause pneumonia, bronchitis, or other problems in the lungs; lead to problems with kidney function; and cause hepatitis or cirrhosis of the liver
- Peripheral neuropathy (numbness, tingling, and burning of the hands and feet)
Risk factors
- Age >40 years
- Female gender
- Rheumatic disease (i.e., rheumatoid arthritis or lupus)
Pathophysiology
Treatment
- Medications
- Decrease eye inflammation (artificial tears): Cyclosporine or lifitegrast
- Increase production of saliva (and sometimes tears): Pilocarpine and cevimeline
- Address specific complications: NSAIDs or other arthritis medications, antifungal medications for yeast infections
- Surgery to seal the nasolacrimal ducts that drain tears from the eyes
Management
Preoperative management
- Complete medical history: Evolution and symptomatology of the disease
- Thorough physical examination
- Continue chronic therapy until the morning of surgery
Intraoperative management
- Goal: Humidify the mucous membranes rigorously during the anesthetic procedure
- Lubricate the eyes to prevent corneal damage
- Avoid respiratory dryness by using humidified oxygen
- Suction efficiently to prevent mucous plugs
- Avoid parasympatholytic and anticholinergic drugs due to their decrease in gland secretions
Postoperative management
- No increased risk for postoperative complications
Suggested reading
- Sjögren Syndrome. In: Bissonnette B, Luginbuehl I, Marciniak B, Dalens BJ. eds. Syndromes: Rapid Recognition and Perioperative Implications. McGraw Hill; 2006. Accessed February 20, 2023. https://accessanesthesiology.mhmedical.com/content.aspx?bookid=852§ionid=49518220
Clinical updates
Aiello et al. (BMC Musculoskeletal Disorders, 2025) report that Sjögren’s syndrome can involve the temporomandibular joint, causing pain, stiffness, and reduced mouth opening, often as part of broader rheumatic disease involvement. This has direct anesthetic implications, as TMJ arthritis may increase the risk of difficult airway management and warrants careful preoperative airway assessment in addition to standard measures for mucosal dryness.











