
 Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Identify the causes leading to delayed emergence
- Explain the risk factors associated with an increased risk of delayed emergence
- Manage delayed emergence
Definition and mechanism
- Failure to regain consciousness or alertness following general anesthesia after surgery
- The transition from unconsciousness to complete wakefulness occurs along a normal trajectory, although slowed down
- Alternatively, the awakening trajectory proceeds abnormally, possibly leading to emergence delirium
- Most cases of delayed return of consciousness are rapidly treatable
Causes
| Pharmacodynamic causes | Genetic variations Hypothermia Drug interaction Serotonin syndrome Neuromuscular blockers Heroin or opioid toxicity IV anesthetic agents (Total intravenous anesthesia (TIVA)) Central anticholinergic syndrome |
| Metabolic alterations | Hypoglycemia Hyperglycemia Hyponatremia Hypernatremia Metabolic acidosis |
| Neurological rare causes | Hypoperfusion/ischemia Intracranial hemorrhage Venous thromboembolism Seizures Myxedema coma Functional coma Brainstem stroke |
| Psychiatric rare causes | Conversion disorder |
Risk factors
| Patients conditions | Older age Body habitus Gender | |
| Preexisting clinical conditions | Psychological disorders Neurologic conditions Cardiac diseases Hypertension Pulmonary diseases Chronic kidney disease Liver diseases Hypothyroidism Drug or alcohol abuse Metabolic alterations | |
| Intraoperative conditions | Drugs (e.g. Heroin or opioid toxicity) Metabolic alterations (intraoperative) | |
| Chronic pharmacotherapy | Benzodiazepines Barbiturates Anticholinergics Antidepressants Antipsychotics Herbal medications |
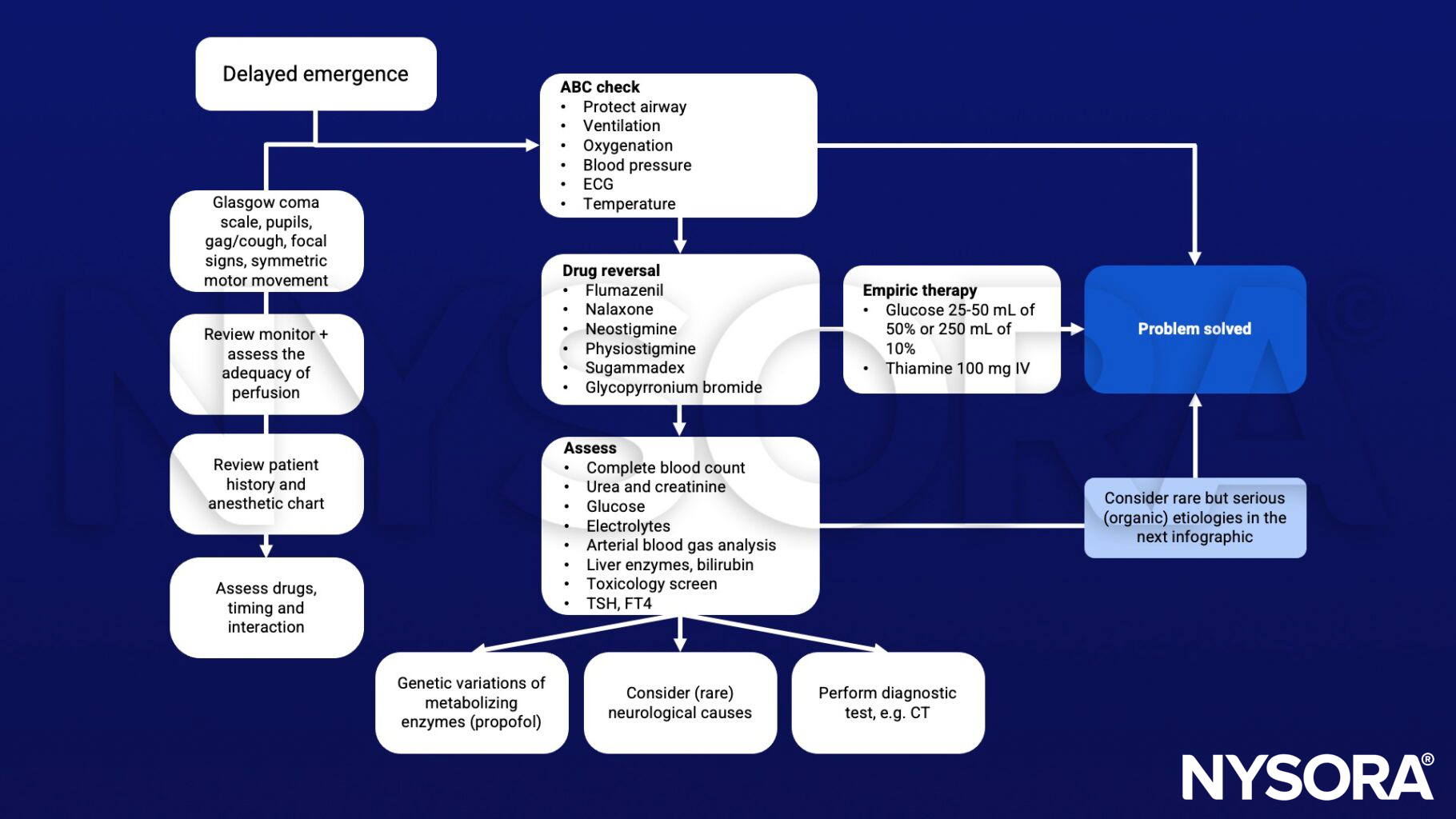
Diagnostic steps
- Vital signs (including temperature)
- neuromuscular monitor
- Neurologic exam (pupils, cranial nerves, reflexes, response to pain)
- Fingerstick glucose
- Arterial blood gas with electrolytes
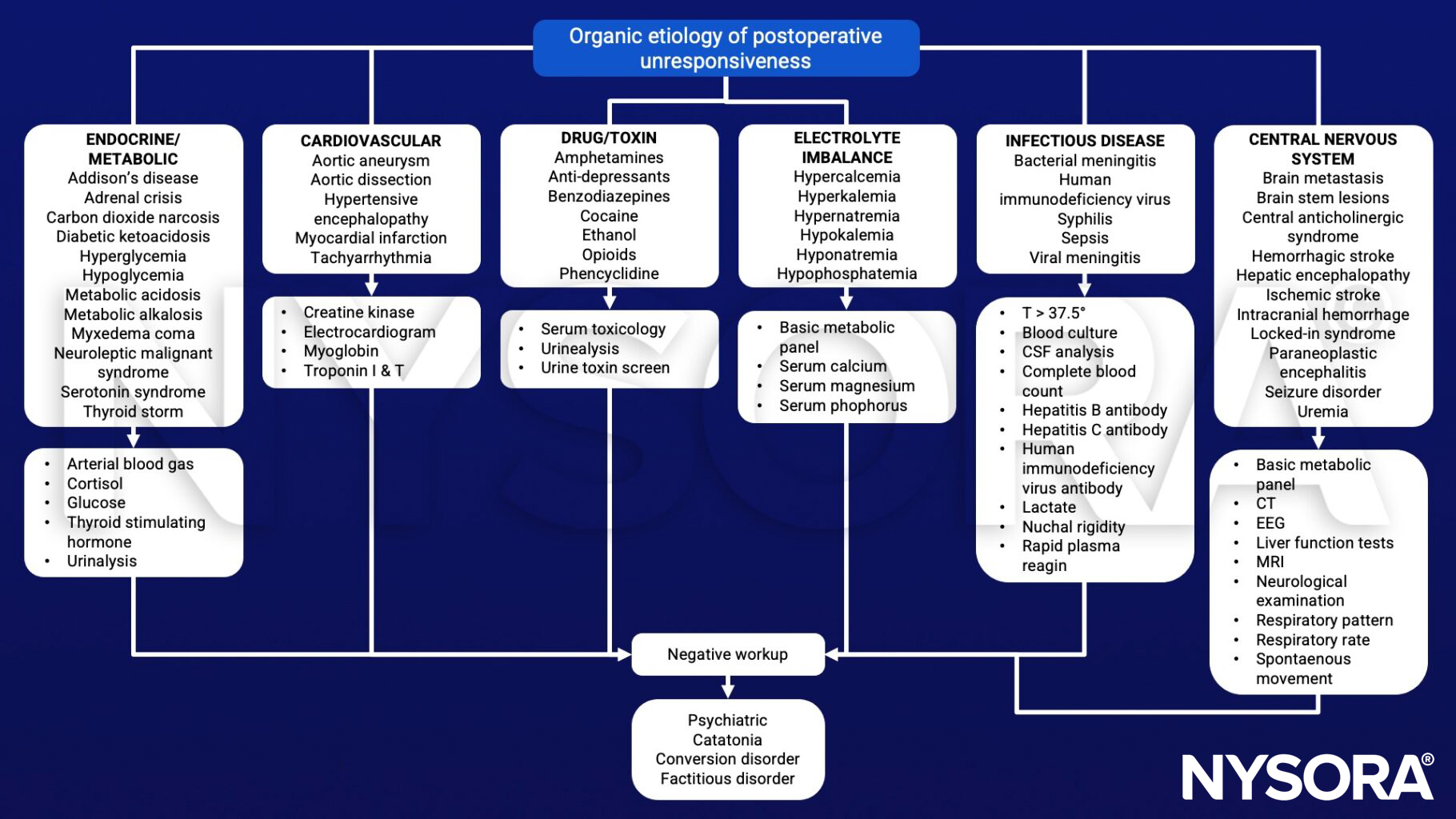
Differential diagnosis
| Drug effects | Residual anesthetic (volatile, propofol, barbiturates, ketamine) Excess narcotics Inadequate reversal or no reversal of muscle relaxation Pseudocholinesterase deficiency Alcohol or street drugs Herbal medicines (valerian root, St. John’s wort) Infection |
| Infection | Encephalitis Meningitis Sepsis |
| Metabolic disorders | Hypercarbia Hypoxemia Metabolic acidosis Acidosis Hypoglycemia/Hyperglycemia Hyponatremia/electrolyte abnormalities Hypothermia/Malignant hyperthermia Uremia Hepatic encephalopathy Osmolality problems Myxedema coma |
| Neurologic disorders | New ischemic event Subarachnoid hemorrhage Seizures or postictal state Increased intracranial pressure or pre-existing obtundation Perioperative stroke (ischemic or hemorrhagic) Hydrocephalus Diffuse anoxic injury Pneumocephalus Cerebral hyperperfusion syndrome |
Management
Additional facts
- Recent studies indicate that induction and awakening are asymmetric processes
- Neural circuits that mediate induction do not completely overlap those that mediate emergence for anesthesia
Suggested reading
- Cascella M, Bimonte S, Di Napoli R. Delayed Emergence from Anesthesia: What We Know and How We Act. Local Reg Anesth. 2020 Nov 5;13:195-206.
- Thomas E, Martin F, Pollard B. Delayed recovery of consciousness after general anaesthesia. BJA Educ. 2020 May;20(5):173-179.
- Rafizadeh S, Kerry-Gnazzo AR, DeWalt K. An Unresponsive Patient in Postanesthesia Care Unit: A Case Report of an Unusual Diagnosis for a Common Problem. A A Pract. 2020 Aug;14(10):e01293.
- Yonekura H, Murayama N, Yamazaki H, Sobue K. A Case of Delayed Emergence After Propofol Anesthesia: Genetic Analysis. A A Case Rep. 2016 Dec 1;7(11):243-246.
Clinical updates
Vetter et al. (European Journal of Anaesthesiology, 2025) report in a single-center RCT of carotid endarterectomy patients that co-administration of dexmedetomidine with TIVA reduced propofol effect-site concentrations required for burst suppression by 33% and decreased vasopressor requirements by 50%, without impairing neurophysiologic monitoring. Importantly, dexmedetomidine did not increase delayed emergence, with comparable postoperative GCS scores and no difference in delirium rates between groups. These findings suggest that dexmedetomidine’s propofol-sparing effect may enhance hemodynamic stability without prolonging recovery, supporting its integration into high-risk neurovascular anesthesia protocols.
- Read more about this study HERE.











