
 Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Recognize the signs of POD
- Identify risk factors for POD
- Reduce the risk of POD in susceptible patients
- Manage POD occurrence
Definition
- Postoperative delirium (POD) is defined as an acute onset fluctuating change in mental status characterized by reduced awareness of the environment and disturbance of attention
- It is a temporary neurocognitive syndrome observed after surgery
- Incidence in older surgical patients varies from 7% to 53%
- POD prolongs postoperative ventilation, intensive care, length of stay, increases costs, and negatively impacts functional outcome and survival
Signs
3 subtypes:
- Hyperactive: Restlessness, agitation, and hypervigilance, often hallucinations and delusions
- Hypoactive: Lethargy and sedation, slow response to questioning, little spontaneous movement
- Mixed: Both hyperactive and hypoactive features
Risk factors
| Predisposing | Precipitating |
|---|---|
| Advanced age | ICU admission |
| Male sex | High-risk surgical procedure |
| Low body mass index | Sleep deprivation |
| Sight/hearing loss | Polypharmacy |
| Social isolation | Medications |
| Multimorbidity | Severe illness (e.g. infection, fracture, stroke) |
| Prior cognitive impairment | Hyper- or hypothermia |
| Malnutrition | Sensory deprivation |
| Low serum albumin | Increasing duration of surgery |
| Frailty | Urgency of surgery |
| Cancer | Pain |
| Alcohol/drug abuse | Perioperative complications |
| Antipsychotics | Hypoxia |
| Malnutrition | Physical restraints |
| Dehydration | Prolonged use of catheters |
| Depression | |
Prevention
- Identify risk factors
- Frailty assessment
- Bispectral index (BIS) monitoring (Target BIS 40-60)
- Avoid benzodiazepines
- Multi-component interventions (visual and hearing aids, sleep promotion, minimalization of catheters/cannulae…)
- Regional anesthesia instead of general
- Treat pain (multimodal strategy)
- Prehabilitation programs that improve physical and cognitive capacity
Preventative measures requiring further investigation:
- Total intravenous anesthesia (TIVA)
- Lighter sedation
- Dexmedetomidine
- Melatonin
- Steroids
- Cholinergic stimulation
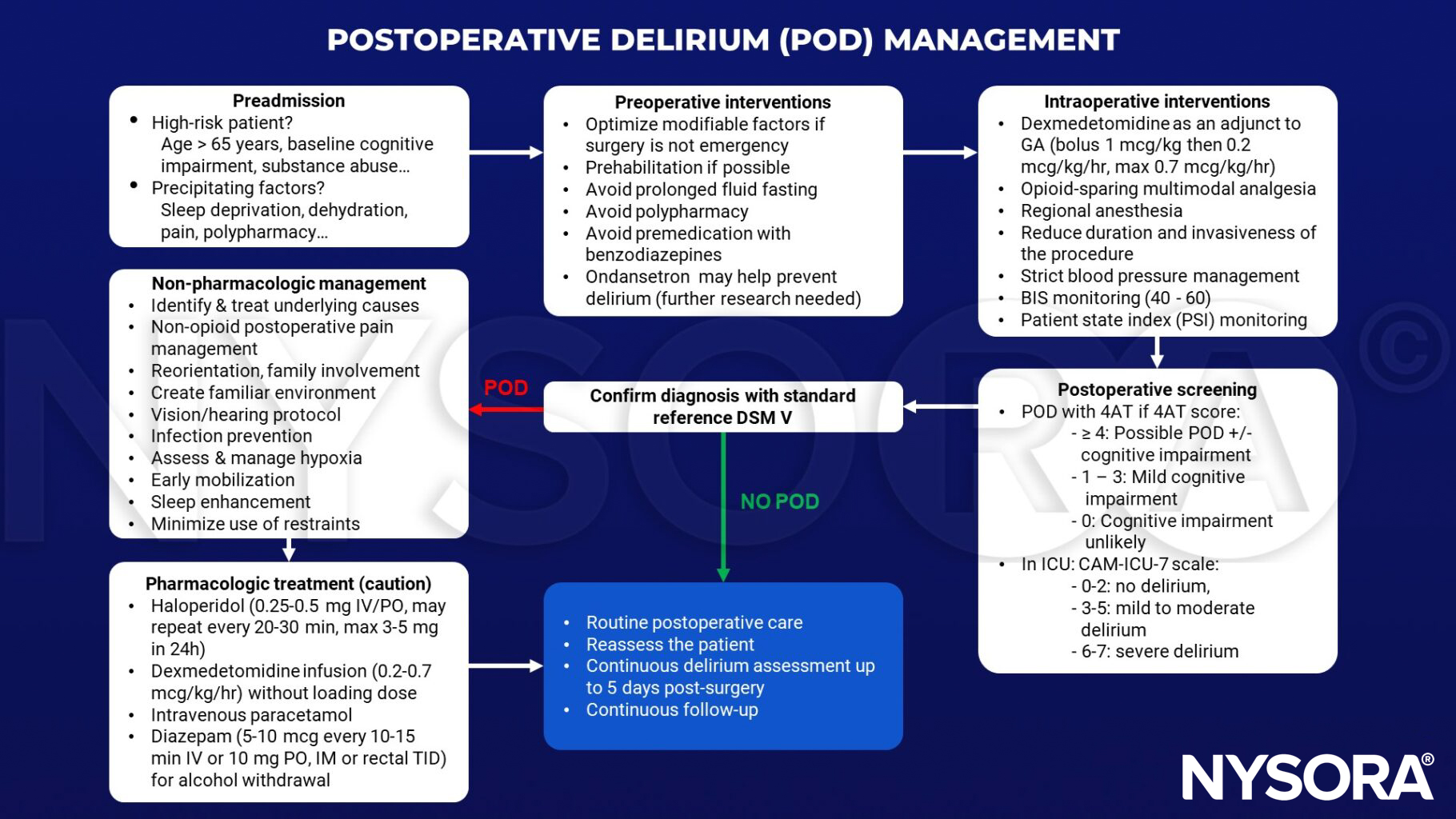
Management
Suggested reading
- Hoogma, Danny Feike; Milisen, Koen; Rex, Steffen; Al tmimi, Layth. Postoperative delirium: identifying the patient at risk and altering the course: A narrative review. European Journal of Anaesthesiology and Intensive Care 2(3):p e0022, June 2023.
- Mossie A, Regasa T, Neme D, Awoke Z, Zemedkun A, Hailu S. Evidence-Based Guideline on Management of Postoperative Delirium in Older People for Low Resource Setting: Systematic Review Article. Int J Gen Med. 2022;15:4053-4065.
- Swarbrick CJ, Partridge JSL. Evidence-based strategies to reduce the incidence of postoperative delirium: a narrative review. Anaesthesia. 2022;77 Suppl 1:92-101.
- Subramaniam B, Shankar P, Shaefi S, et al. Effect of Intravenous Acetaminophen vs Placebo Combined With Propofol or Dexmedetomidine on Postoperative Delirium Among Older Patients Following Cardiac Surgery: The DEXACET Randomized Clinical Trial [published correction appears in JAMA. 2019 Jul 16;322(3):276]. JAMA. 2019;321(7):686-696.
- Haque N, Naqvi RM, Dasgupta M. Efficacy of Ondansetron in the Prevention or Treatment of Post-operative Delirium-a Systematic Review. Can Geriatr J. 2019;22(1):1-6. Published 2019 Mar 30.
- Khan BA, Perkins AJ, Gao S, et al. The Confusion Assessment Method for the ICU-7 Delirium Severity Scale: A Novel Delirium Severity Instrument for Use in the ICU. Crit Care Med. 2017;45(5):851-857.
- Chan MT, Cheng BC, Lee TM, Gin T; CODA Trial Group. BIS-guided anesthesia decreases postoperative delirium and cognitive decline. J Neurosurg Anesthesiol. 2013;25(1):33-42.
- Fong TG, Tulebaev SR, Inouye SK. Delirium in elderly adults: diagnosis, prevention and treatment. Nat Rev Neurol. 2009;5(4):210-220.
- Robinson TN, Eiseman B. Postoperative delirium in the elderly: diagnosis and management. Clin Interv Aging. 2008;3(2):351-355.
Clinical updates
Aldecoa et al. (EJA, 2024) update the European Society of Anaesthesiology and Intensive Care (ESAIC) guidelines on postoperative delirium (POD), emphasizing mandatory preoperative risk screening for patients ≥ 60 years and implementation of structured, multicomponent nonpharmacological prevention bundles as the cornerstone of care. The guideline highlights neuroinflammation, blood–brain barrier disruption, and neurotransmitter imbalance as central mechanisms, supports selective use of dexmedetomidine in high-risk patients, and discourages routine use of haloperidol, cholinesterase inhibitors, biomarker screening, or reliance on anesthetic technique alone. These updates reinforce that effective POD prevention depends on early risk stratification, multidisciplinary coordination, and standardized postoperative monitoring rather than isolated pharmacologic interventions.
Ahrens et al. (A&A, 2025) analyzed 53,772 patients aged ≥ 60 years and found that intraoperative use of nondepolarizing neuromuscular blocking agents (ND-NMBAs) was associated with a dose-dependent increase in postoperative delirium, with each ED95 increment linked to a 9% higher risk and no-reversal cases showing a 52% increased odds of delirium. Importantly, this association was no longer significant when neuromuscular blockade was appropriately reversed with neostigmine or sugammadex, with no difference between reversal agents. These findings identify residual neuromuscular blockade as a modifiable perioperative risk factor for POD and support routine quantitative monitoring and pharmacologic reversal in older surgical patients.
Rössler et al. (Anesthesiology, 2025) analyzed 38,940 noncardiac surgeries and found that intraoperative hypotension, defined as MAP < 65 mmHg, was not independently associated with postoperative delirium (POD), challenging the long-held assumption that this threshold directly drives delirium risk. Instead, postoperative blood pressure showed a U-shaped association: both lower MAP and MAP > 88 mmHg were linked to higher delirium incidence, and increased postoperative blood pressure variability (ARV, VIM) showed a nonlinear relationship with POD. These findings suggest that postoperative hemodynamic stability and avoidance of excessive BP variability may be more clinically relevant for POD prevention than strict intraoperative MAP targets alone.
- Read more about this study HERE.
Bruzzone et al. (A&A, 2025) systematically reviewed 55 studies and found that intraoperative EEG markers are consistently associated with a higher risk of postoperative delirium (POD), whereas preoperative EEG findings were inconsistent predictors. Postoperatively, delirious patients demonstrated EEG slowing and disrupted functional connectivity, reinforcing EEG-defined cortical hypoactivity as a biological correlate of POD. These findings position intraoperative EEG monitoring, especially avoidance of excessive burst suppression, as a promising strategy for identifying and potentially mitigating POD risk in older surgical patients.
- Read more about this study HERE.
An investigator-initiated randomized controlled trial published in Anesthesiology (2026) reports that perioperative S-ketamine significantly reduces postoperative delirium in elderly patients undergoing total hip or knee arthroplasty under neuraxial anesthesia. In 372 patients ≥ 60 years, S-ketamine reduced 3-day POD incidence from 20.4% to 8.1% and improved postoperative day 1 pain during mobilization. Neuropsychiatric adverse effects (e.g., nightmares, hallucinations) were infrequent and transient, supporting S-ketamine as a potentially effective delirium-prevention strategy when GABAergic sedation is avoided.
- Read more about this study HERE.












