Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Outline the signs and symptoms of jaundice
- Describe the causes of jaundice and their classification
- Anesthetic management of a jaundiced patient
Definition and mechanisms
- Jaundice, or icterus, is a yellowish discoloration of the skin and sclera due to high bilirubin levels
- Jaundice in adults indicates the presence of underlying diseases involving abnormal heme metabolism, liver dysfunction, or biliary tract obstruction
- Surgery should be avoided in these patients, only emergency procedures
Signs and symptoms
- Hyperbilirubinemia (serum bilirubin ≥3 mg/dL)
- Yellowish discoloration of the skin, mucous membranes, and sclera
- Itchiness (pruritus)
- Pale fatty stool (steatorrhea)
- Dark urine (bilirubinuria)
- Abdominal pain
- Fatigue
- Weight loss
- Vomiting
- Fever
Complications
- Hyperbilirubinemia-induced neurological damage → kernicterus (especially in newborns)
- Coagulopathy
- Vitamin K-dependent coagulation factors (II, VII, IX, and X) are reduced, resulting in a prolonged prothrombin time
- Hepatocellular coagulopathy is often refractory to vitamin K administration
- Disseminated intravascular coagulation (DIC) is associated with secondary biliary tract infection
- Altered drug handling
- Drugs excreted via the biliary system have prolonged elimination half-life in cholestasis
- Atracurium is the drug of choice for muscular relaxation
- Acute oliguric renal failure (17%)
- Stress ulceration with gastrointestinal hemorrhage (16%)
- Reduced wound healing
Causes
| Category | Definition | Causes |
|---|---|---|
| Prehepatic/hemolytic | Pathology occurs prior to liver metabolism, due to increased breakdown of erythrocytes → increased rate of erythrocyte hemolysis → increased unconjugated serum bilirubin → increased deposition of unconjugated bilirubin into mucosal tissue | Sickle-cell anemia Spherocytosis Thalassemia Pyruvate kinase deficiency Glucose-6-phosphate dehydrogenase deficiency Microangiopathic hemolytic anemiaanemia Hemolytic-uremic syndrome Severe malaria |
| Hepatic/hepatocellular | Pathology is due to damage of parenchymal liver cells → abnormal liver metabolism of bilirubin | Acute hepatitis Chronic hepatitis Hepatotoxicity Cirrhosis Drug-induced hepatitis Alcoholic liver disease Gilbert syndrome Crigler-Najjar syndrome Leptospirosis |
| Posthepatic/cholestatic (obstructive jaundice) | Pathology occurs after bilirubin conjugation in the liver, due to obstruction of the biliary tract and/or decreased bilirubin excretion | Choledocholithiasis (common bile duct gallstones) Pancreatic cancer of the pancreatic head Biliary tract strictures Biliary atresia Primary biliary cholangitis Cholestasis of pregnancy Acute pancreatitis Chronic pancreatitis Pancreatic pseudocysts Mirizzi syndrome Parasites |
Risk factors
- Male gender
- White ethnicities
- Active smoking
Treatment
- Based on the underlying cause
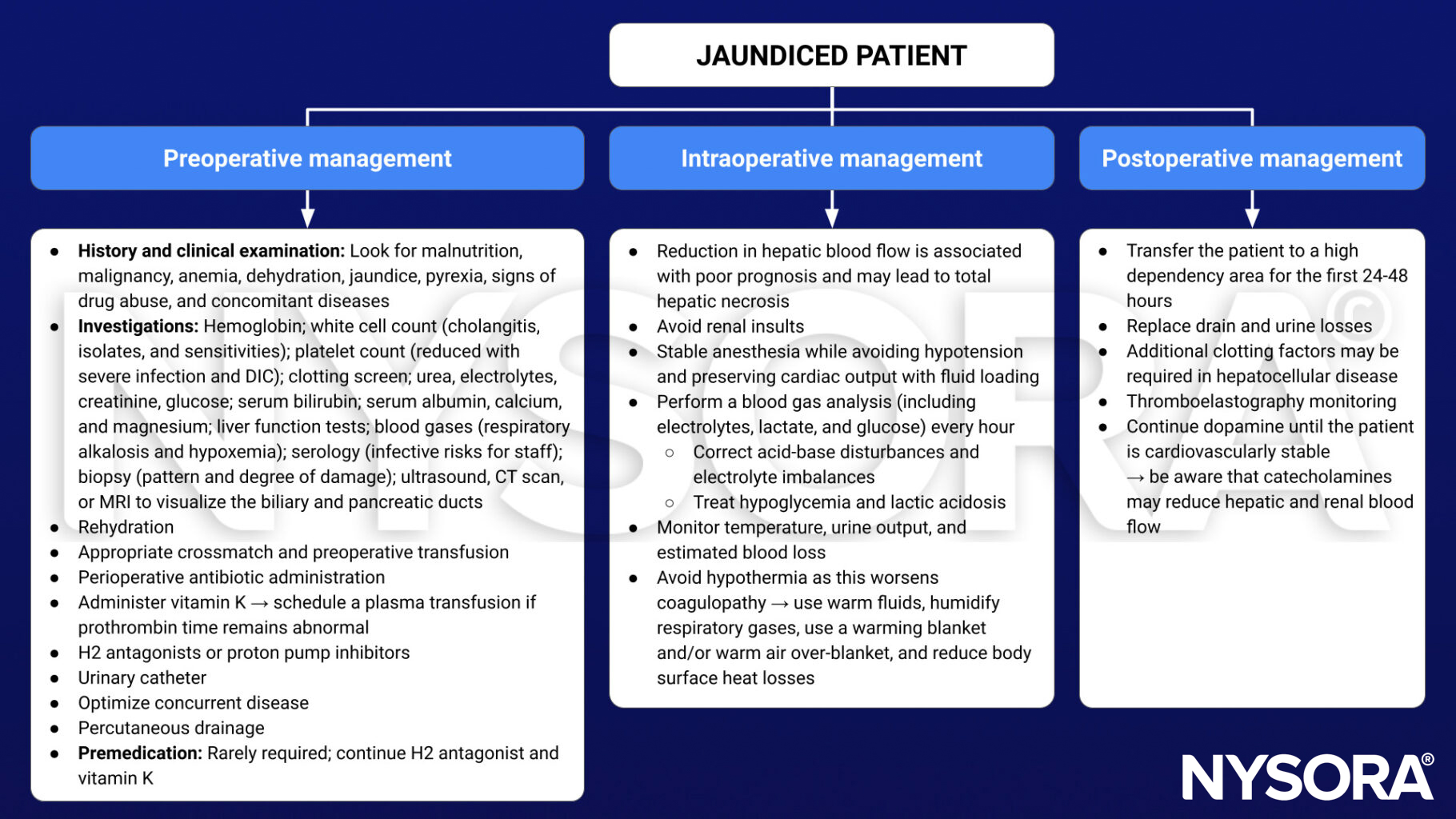
Management
Suggested reading
- Pollard BJ, Kitchen G. Handbook of Clinical Anaesthesia. 4th ed. Taylor & Francis group; 2018. Chapter 4 Gastrointestinal tract, Jackson MJ.
- Wang L, Yu W. Obstructive jaundice and perioperative management. Acta Anaesthesiol Taiwan. 2014;52(1):22-29.
Clinical updates
Li et al. (Medicine, 2025) report that obstructive jaundice significantly alters the pharmacodynamics of commonly used anesthetic agents, with increased sensitivity and reduced requirements for inhaled anesthetics (e.g., desflurane), etomidate, opioids, and rocuronium, while propofol and atracurium/cisatracurium are relatively unaffected. These findings underscore the need for careful agent selection, dose reduction, and vigilant neuromuscular and hemodynamic monitoring in jaundiced patients to minimize perioperative hypotension, prolonged neuromuscular blockade, and postoperative complications.