
- Learn
-
Apps
View all apps
Veterinary
 VetRA App
VetRA App

- Books
- Events
- News
- Partners
- About
- For Clinicians
 VetRA App
VetRA App
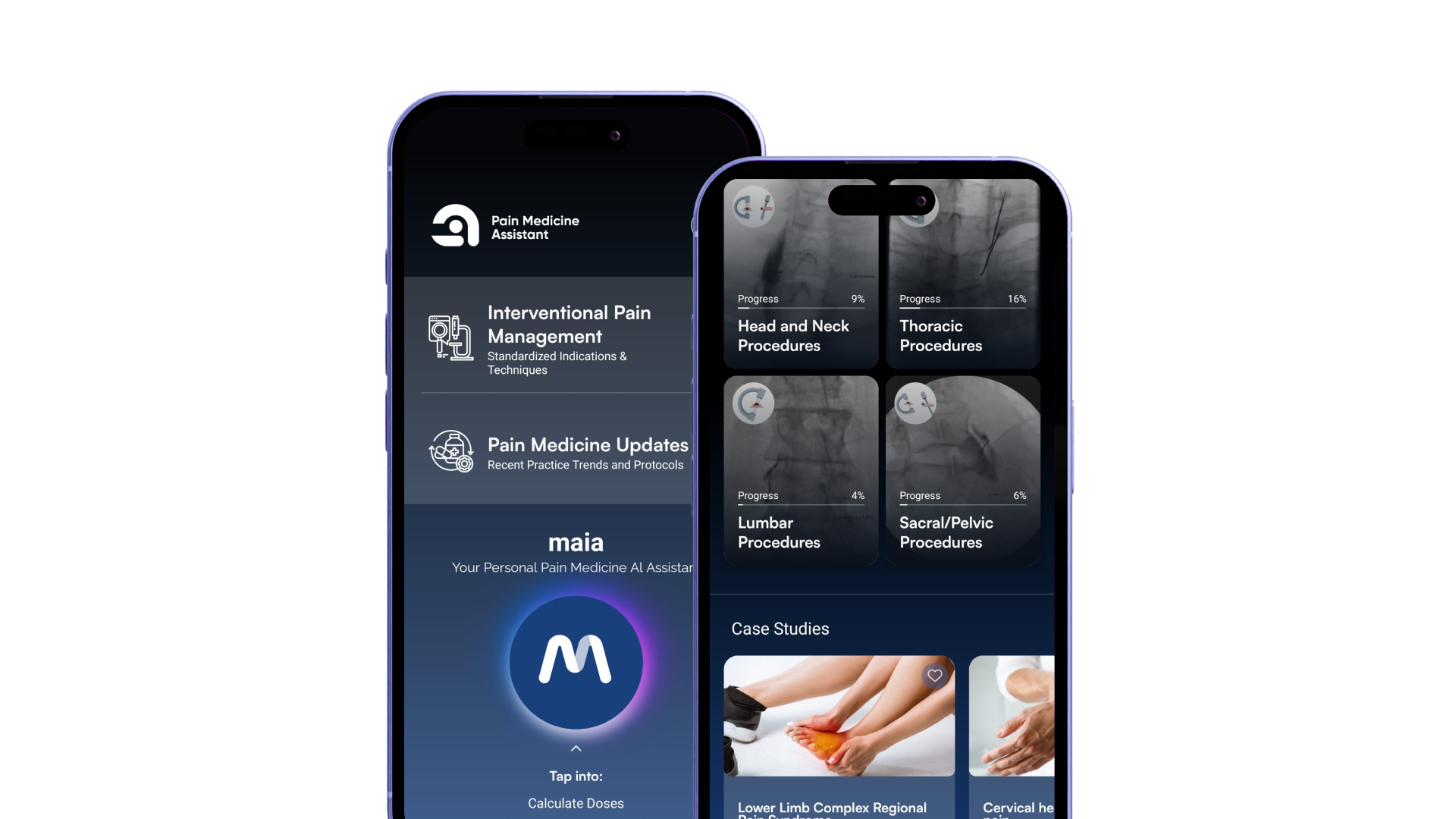
Structured reference for chronic pain procedures, standardized techniques, literature updates, and AI-powered support - right at your fingertips.



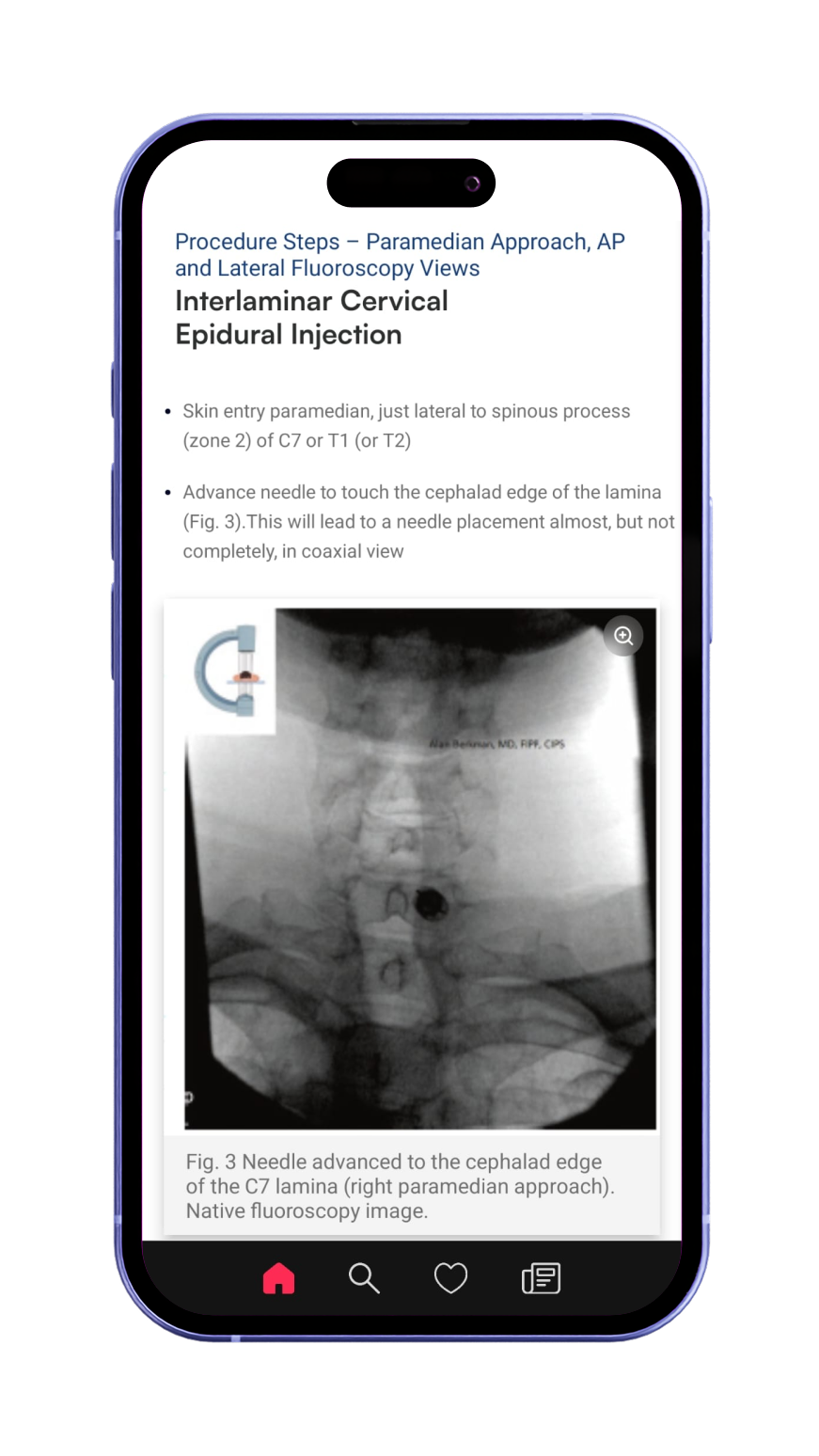
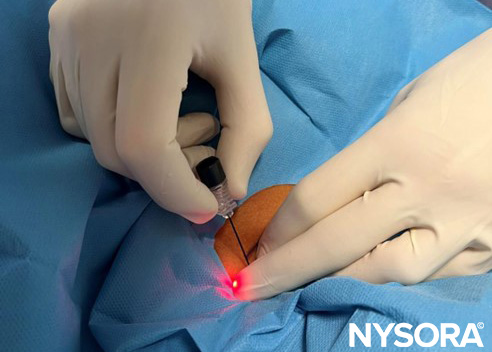
From patient positioning to injection.
With Pain Medicine Updates.
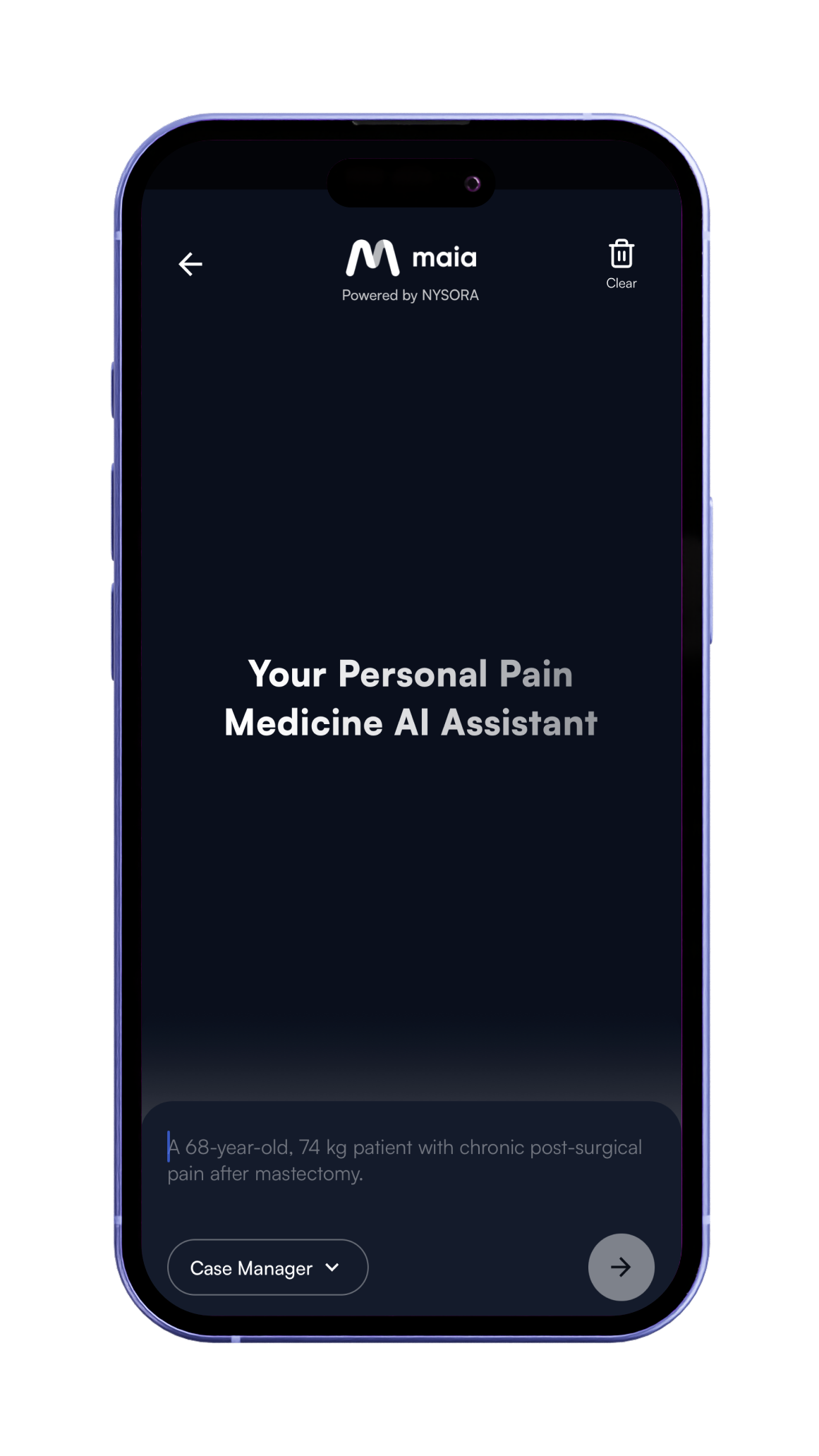
MAIA supports clinical decision-making.
From patient positioning to injection.
With Pain Medicine Updates.
MAIA supports clinical decision-making.

The first mobile AI-supported guide for pain medicine. Trusted by pain physicians and students worldwide.



For this pediatric anesthesiologist, reaching the top of the Daily Question rankings in the NYSORA Nerve Blocks App was not simply about knowing the right answers. It was part of a much larger habit: continually learning, reviewing, and bringing new ideas into clinical practice. When the July Daily Question rankings closed, one name stood at the top: Mihaela Visoiu. Naturally, we wanted to meet the clinician behind the result. Who was answering these questions each day? What kept her coming back? And, perhaps more importantly, how did this brief daily activity fit into the much more demanding reality of clinical practice? Mihaela’s answers revealed that her place at the top of the rankings was not the result of competition alone. It reflected the way she approaches regional anesthesia: with curiosity, consistency, and a willingness to keep revisiting even familiar techniques. A career centered on pediatric regional anesthesia Mihaela is a pediatric anesthesiologist at UPMC Children’s Hospital of Pittsburgh in Pennsylvania, where her work extends across the operating room, perioperative pain management, and education. Her clinical responsibilities include providing general and regional anesthesia, managing perioperative pain, rounding on hospitalized patients, and teaching student nurse anesthetists, residents, and fellows. Her particular interest is pediatric regional anesthesia – especially ultrasound-guided nerve blocks in neonates, infants, and children. Even with years of experience, Mihaela does not view learning as something that ends once a technique becomes familiar. “I want to learn additional techniques for performing these blocks and better understand how they compare with established approaches to perioperative pediatric pain management.” That mindset – looking beyond the technique she already knows – is central to how she uses the NYSORA Nerve Blocks App. From a NYSORA conference to a clinical reference Mihaela first discovered the app after attending a NYSORA conference in New York […]
Thoracic paravertebral block remains the preferred regional analgesic technique for video-assisted thoracoscopic surgery, according to a new randomized non-inferiority trial. While intrathecal morphine provided comparable pain scores and recovery quality, it failed to demonstrate non-inferiority for reducing postoperative opioid consumption, reinforcing current guideline recommendations. Video-assisted thoracoscopic surgery still presents a significant pain management challenge Video-assisted thoracoscopic surgery (VATS) has transformed thoracic surgery by reducing tissue trauma, shortening hospital stays, and accelerating postoperative recovery compared with open thoracotomy. Nevertheless, postoperative pain remains a major clinical concern. Moderate-to-severe pain affects nearly two-thirds of patients undergoing VATS. Poorly controlled pain impairs coughing, deep breathing, sputum clearance, and early mobilization while increasing the risk of pulmonary complications and chronic postsurgical pain. Modern Enhanced Recovery After Surgery (ERAS) pathways emphasize multimodal analgesia, combining systemic medications with regional anesthesia techniques to minimize opioid exposure while maintaining excellent pain control. Among available regional techniques, thoracic paravertebral block (TPVB) is widely recommended. However, intrathecal morphine (ITM) offers several practical advantages, including technical simplicity, single-shot administration, and broad availability in hospitals where ultrasound-guided regional anesthesia expertise may be limited. Until now, robust head-to-head evidence comparing these two strategies has been limited. New randomized trial compares two commonly used analgesic techniques Researchers conducted a prospective randomized observer-blinded non-inferiority trial evaluating postoperative analgesia after elective VATS. Study design The investigators enrolled: 72 adult patients undergoing elective VATS ASA physical status I–III Randomized 1:1 36 patients received thoracic paravertebral block 36 patients received intrathecal morphine Two patients converted from VATS to thoracotomy and were excluded from the per-protocol analysis. Regional anesthesia protocols Thoracic paravertebral block Ultrasound-guided T5 level 0.25% bupivacaine Epinephrine added Intrathecal morphine Lumbar spinal injection Morphine dose: 5 μg/kg Based on ideal body weight All patients received identical general anesthesia, multimodal postoperative analgesia, and morphine patient-controlled analgesia (PCA). Primary outcome […]

The first mobile AI-supported guide for pain medicine. Trusted by pain physicians and students worldwide.
The app includes:
The NYSORA Pain Medicine Assistant App provides on-the-go access to expertly-curated techniques, helping you:
The app covers:
The app can be used in multiple ways:
It’s a mobile-friendly reference tool offering:
 Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About