Learning objectives
- Describe the overall mechanisms of AF
- Recognize risk factors for perioperative AF
- Manage patients with AF or risk of AF
Definition & mechanisms
- Atrial fibrillation (AF) is the most common sustained arrhythmia
- Very rapid and uncoordinated atrial activity
- Twofold increase in premature mortality
- Important factor in major adverse cardiovascular events such as heart failure, severe stroke, and myocardial infarction
- Initiation and maintenance of AF can be linked to “trigger” (initiating event) and “substrate” (atrial remodeling that maintains AF)
- Risk of congestive heart failure, embolic events, stroke
Risk factors for perioperative AF
| Patient-related | Surgery-related |
|---|---|
| Age | Hypovolemia and hypervolemia |
| Race (lower risk in African population) | Hypoxia |
| History of atrial fibrillation | Intraoperative hypotension |
| Congestive heart failure | Catecholamine versus noncatecholamine vasopressor use |
| Ischemic heart disease | Trauma |
| Hypertension | Pain |
| Chronic renal failure | Type of surgery |
| Sepsis | Hypoglycemia |
| Asthma | Electrolyte abnormalities (primarily hypokalemia and hypomagnesemia) |
| Cardiac valvular disease | Anemia |
| Obstructive sleep apnea |
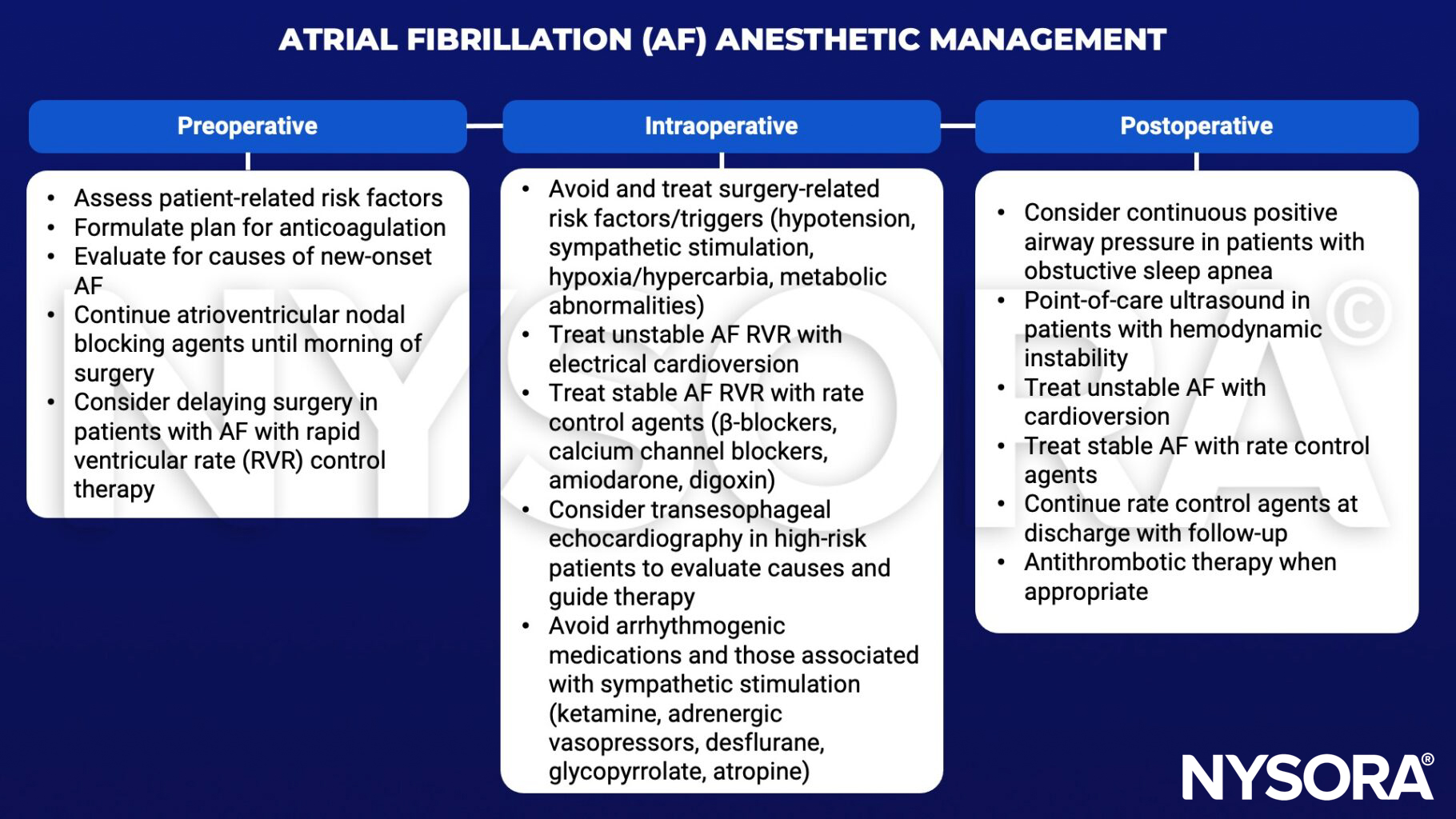
Management
Keep in mind
- Patients who develop perioperative AF have higher in-hospital mortality and longer hospital lengths of stay
- Those with preexisting AF who develop perioperative AF have similar outcomes compared with patients who develop perioperative AF de novo
Suggested reading
- Karamchandani K, Khanna AK, Bose S, Fernando RJ, Walkey AJ. Atrial Fibrillation: Current Evidence and Management Strategies During the Perioperative Period. Anesthesia & Analgesia. 2020;130(1).
- Wijesurendra RS, Casadei B. Mechanisms of atrial fibrillation. Heart. 2019;105(24):1860-1867
Clinical updates
Suleiman et al. (BJA, 2025) review updated evidence on perioperative management of direct oral anticoagulants (DOACs), commonly prescribed for atrial fibrillation, around neuraxial and deep peripheral nerve block procedures, highlighting differences between the 2025 ASRA guidelines and the PAUSE protocol. ASRA recommends a more conservative interruption and selective DOAC level testing, whereas the PAUSE strategy supports shorter 2-day interruptions without routine testing; pilot PAUSE-2 data show ~95% of patients achieve target DOAC levels with a 25% shorter interruption and no signal of increased bleeding, though rare spinal hematoma risk remains underpowered. These findings suggest that in atrial fibrillation patients, individualized DOAC interruption strategies may safely expand access to neuraxial anesthesia while maintaining thromboembolic protection.
- Read more about this study HERE.