

Learning objectives
- Describe the risk factors for PMI
- Give prophylactic treatment to high-risk patients
- Manage PMI cases
Definition & mechanisms
- Postoperative myocardial injury/infarction (PMI) is a common complication after non-cardiac surgery
- PMI is defined as the increase of troponin caused by ischemia within 30 days after surgery
Pathophysiology
- Type I MI: plaque destruction followed by coronary atherosclerotic thrombosis
- Type II MI: Imbalance in myocardial oxygen supply and demand resulting in ischemia
Risk factors
| Patient-specific | Previous coronary artery disease |
| Age >70 years | |
| Female sex | |
| Renal failure | |
| Diabetes | |
| Peripheral artery disease | |
| Emergency or redo surgery | |
| Severe LV dysfunction (LVEF<35%) or cardiogenic shock | |
| Intraoperative | Open surgery |
| Prolonged intraoperative time with hypotension | |
| Intraoperative heart rate of >110 or <55 BPM | |
| Tachycardia | |
| Intraoperative transfusions | |
| Perioperative vasopressors | |
| Postoperative | Postoperative bleeding |
| Sepsis | |
| Hypoxia | |
| Sustained tachycardia | |
| Hypotension | |
| Severe anemia |
Prophylaxis
- β-adrenergic blockers
- Calcium channel blockers
- α2 agonists
- Statins
- Aspirin
- Coronary revascularization (requires further investigation)
- Anemia corrections
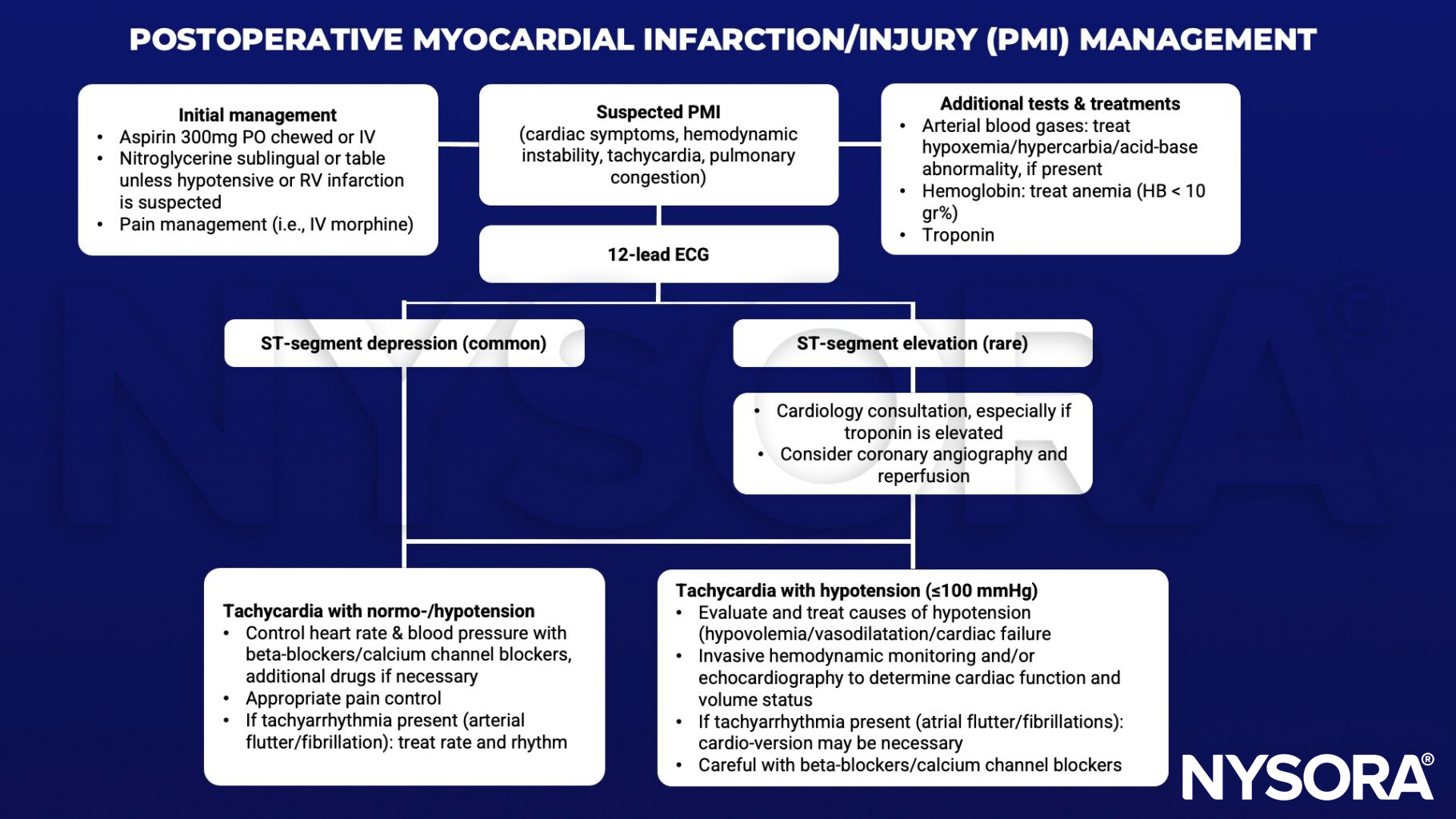
Management
Keep in mind
- Careful perioperative monitoring for ischemia, a low threshold for treating and preventing tachycardia while avoiding hypotension, decreased cardiac output, and/or cardiac decompensation help prevent PMI
- Coronary intervention is rarely indicated as the first line of treatment
- Antithrombotic therapy may exacerbate bleeding
Suggested reading
- Gao L, Chen L, He J, et al. Perioperative Myocardial Injury/Infarction After Non-cardiac Surgery in Elderly Patients. Front Cardiovasc Med. 2022;9:910879.
- Landesberg G, Beattie WS, Mosseri M, Jaffe AS, Alpert JS. Perioperative myocardial infarction. Circulation. 2009;119(22):2936-2944.
- Nashef S., Roques F., Michel P., et al. European system for cardiac operative risk evaluation. Eur J Cardiothorac Surg 1999; 16:9-13
Clinical updates
De Paula–Garcia et al. (Current Opinion in Anaesthesiology, 2025) report that myocardial injury after noncardiac surgery (MINS), defined by isolated postoperative troponin elevation within 30 days, affects ~20% of patients and remains strongly associated with 1-year mortality. The review emphasizes continuing chronic statins and beta-blockers perioperatively, reconsidering routine discontinuation of renin–angiotensin system inhibitors based on recent trials, and selectively maintaining aspirin when bleeding risk is acceptable, while avoiding de novo beta-blocker initiation immediately before surgery. Evidence for intensified post-MINS anticoagulation remains inconclusive, supporting a personalized, multidisciplinary approach with careful hemodynamic monitoring instead.
Wittmann et al. (Current Opinion in Anaesthesiology, 2025) highlight that myocardial injury after noncardiac surgery (MINS) affects ~18–20% of patients, with 84–93% of cases clinically silent and detectable only through routine postoperative troponin surveillance; even minor elevations are associated with increased 1-year mortality. The authors emphasize that MINS is predominantly driven by perioperative oxygen supply–demand mismatch rather than atherothrombosis, supporting strict hemodynamic optimization and routine troponin screening. Pharmacologic prevention remains limited, underscoring the need for individualized secondary prevention and cardiology follow-up.
- Read more about this study HERE.
Giannas et al. (British Journal of Anaesthesia, 2025) report in a mixed-methods analysis that perioperative continuation versus discontinuation of ACE inhibitors/ARBs in major noncardiac surgery showed no difference in mortality or MACE, although withholding therapy reduced intraoperative hypotension but increased acute hypertension. Importantly, emerging data suggest that stopping RAS inhibitors may increase myocardial injury risk in lower-risk patients, and 64.5% of heart failure patients were still advised to stop therapy despite guideline support for continuation. These findings support individualized perioperative RAS management, early postoperative reinitiation, and careful hemodynamic control to mitigate myocardial injury risk.
- Read more about this study HERE.
Zhang et al. (Anesthesiology, 2026) found in a two-center cohort of 1,467 high-risk older adults undergoing hip fracture surgery that postoperative myocardial injury occurred in 12.0% with peripheral nerve block (PNB) versus 21.5% without, with PNB independently associated with a 40% reduction in odds. This study suggests that single-injection PNB, likely via improved pain control and reduced physiologic stress, may mitigate myocardial injury risk.











