Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About

While often silent, Myocardial Injury After Noncardiac Surgery (MINS) significantly increases morbidity and mortality in surgical patients.
This post is based on a recent article by Wittmann et al., published in Current Opinion in Anesthesiology, which explores the latest findings on how to prevent, identify, and manage MINS in surgical patients.
Why This Topic Is Important
Up to 20% of adult surgical patients experience postoperative troponin elevation, yet most have no symptoms. Despite the lack of overt clinical signs, studies show that even small postoperative increases in troponin levels are associated with higher mortality and cardiovascular complications for up to a year after surgery. Given that MINS remains largely undetected without troponin screening, early identification and intervention are critical.
How the Authors Did the Study
Wittmann et al. conducted a narrative review of the latest literature on:
- The definition and epidemiology of MINS
- Potential perioperative triggers that contribute to myocardial injury
- Preventive measures to mitigate risk
- Management strategies that improve patient outcomes
The review analyzed large-scale cohort studies and clinical trials that have shaped our current understanding of MINS, emphasizing its high prevalence, silent nature, and deadly consequences.
What the Authors Found
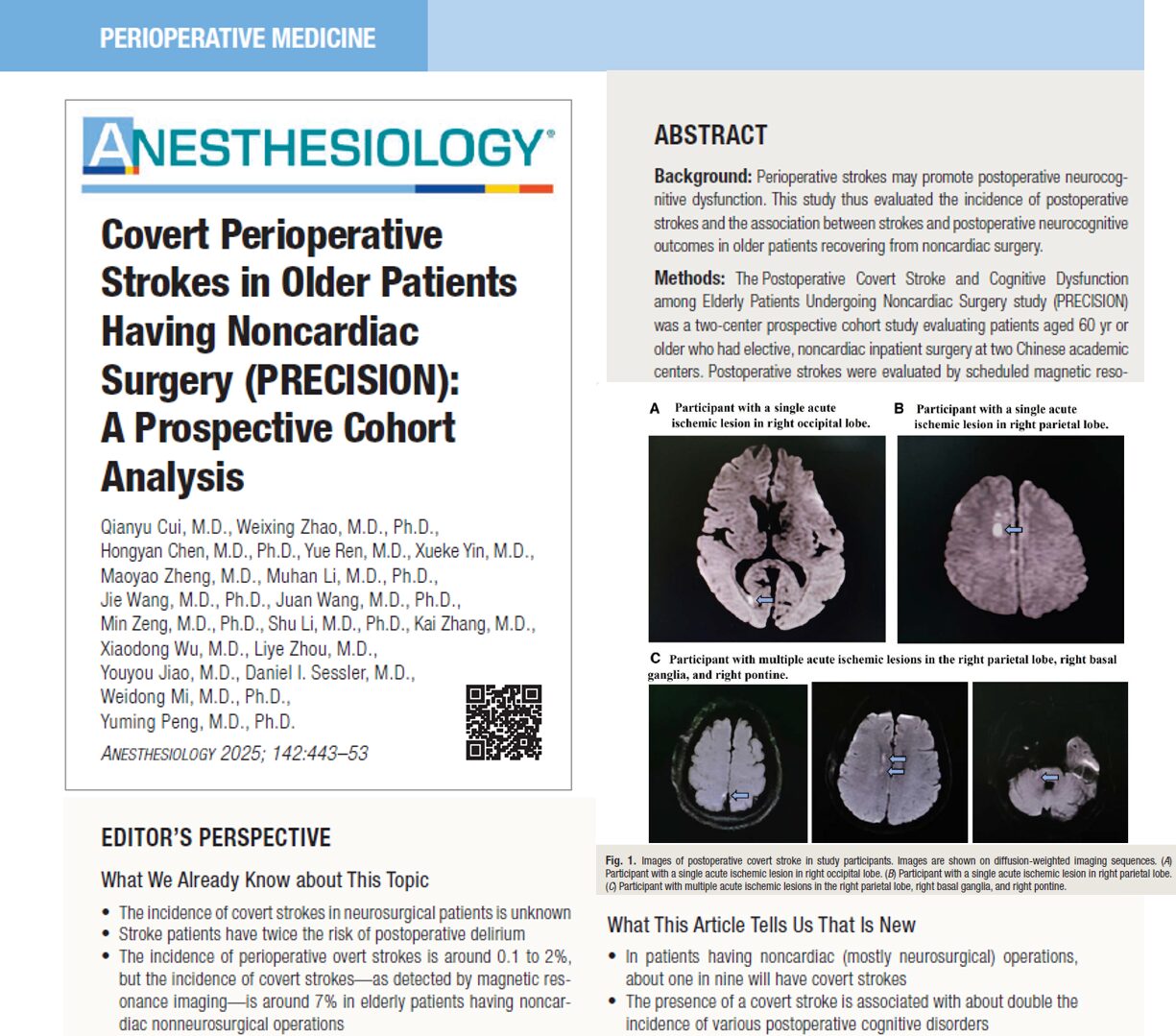
- MINS is widespread yet underdiagnosed
- About 18% of patients in the VISION study (a major perioperative study) had postoperative troponin elevations that met the criteria for MINS.
- 84% of these patients had no symptoms, meaning MINS is often missed without active surveillance.
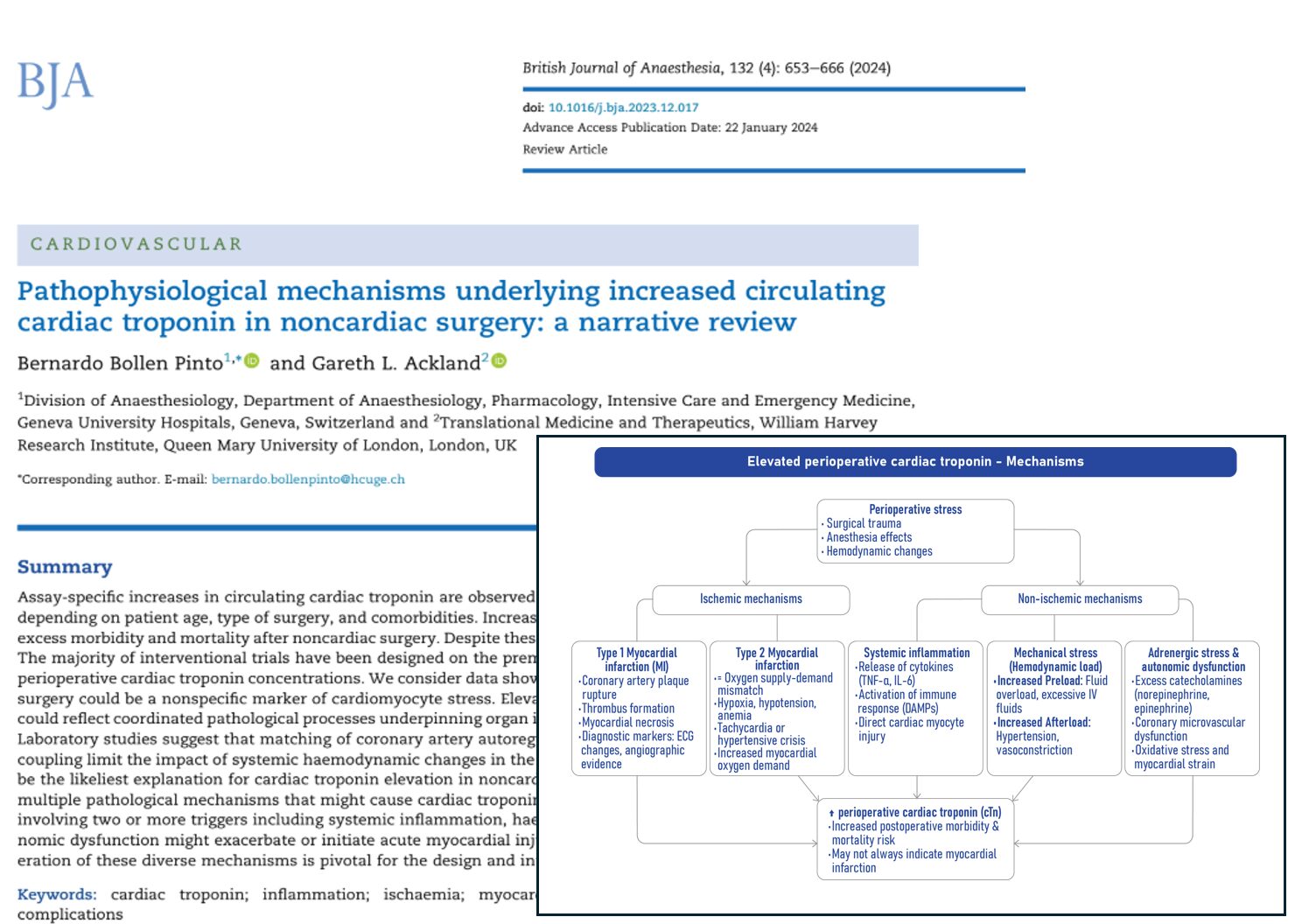
- Common perioperative triggers for MINS
- Hypotension (intraoperative and postoperative)
- Tachycardia and hypertension
- Anemia and inadequate oxygen delivery
- Hypothermia (below 35.5°C)
- Uncontrolled postoperative pain
- Coronary artery disease (pre-existing CAD is present in ~72% of perioperative MIs)
- Postoperative Troponin surveillance is essential
- 93% of MINS cases would be missed without routine troponin screening.
- Serial troponin measurements before and after surgery improve detection and help distinguish acute from chronic elevations.
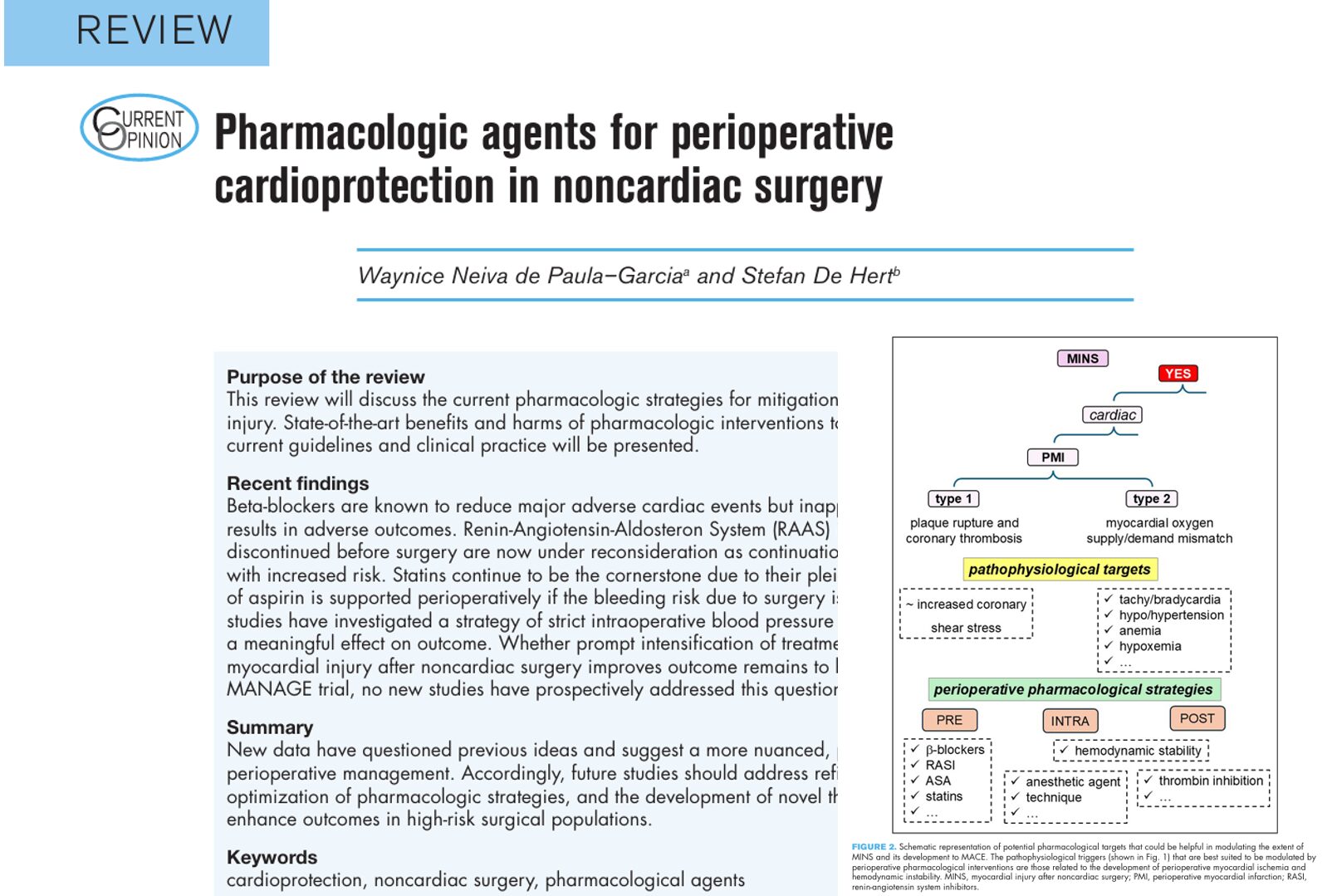
- No single medication prevents MINS, but some reduce risk
- Beta-blockers (POISE trial): Reduced nonfatal MI but increased stroke and mortality, making routine use controversial.
- Aspirin & Clonidine (POISE-2 trial): No significant benefit in reducing MINS.
- Dabigatran (MANAGE trial): Reduced major vascular events in MINS patients but increased bleeding risk.
- Statins & Antiplatelets: Observational studies suggest these drugs may improve outcomes, but more research is needed.
Breaking It Down: Why This Matters
MINS is not simply a postoperative anomaly—it is a predictor of death and major adverse cardiovascular events. Despite its prevalence, MINS lacks clear, standardized management, and many institutions do not routinely screen for it. This is a major gap in perioperative care.
Wittmann et al. emphasize that MINS is more likely caused by supply-demand mismatch rather than atherothrombosis, highlighting the importance of maintaining hemodynamic stability rather than focusing solely on clot prevention.
The takeaway? Anesthesiologists, surgeons, and intensivists must collaborate to actively prevent, identify, and manage MINS in high-risk patients.
Key Takeaways for Clinicians
To prevent and manage MINS, consider these evidence-based strategies:
Preoperative risk stratification
- Identify high-risk patients (e.g., age > 65, preexisting CAD, diabetes, chronic kidney disease).
- Consider baseline troponin and BNP testing for risk assessment.
Intraoperative management
- Avoid hypotension: Keep MAP >65 mmHg using vasopressors when necessary.
- Control tachycardia: Prevent excessive sympathetic activation.
- Maintain normothermia: Hypothermia increases cardiac stress.
- Optimize oxygenation and hemoglobin levels: Liberal transfusion strategies may benefit select high-risk patients.
Postoperative monitoring and management
- Screen troponin levels at 6-12 hours post-op and daily for 2-3 days in high-risk patients.
- Manage pain effectively to reduce catecholamine surges.
- Consider secondary prevention medications (statins, aspirin, anticoagulants) in patients diagnosed with MINS.
- Ensure cardiology follow-up for long-term risk reduction.
Final Thoughts
MINS is a silent but deadly complication that demands proactive surveillance and intervention. Troponin monitoring, hemodynamic stability, and secondary prevention strategies can help improve patient outcomes and reduce perioperative mortality.
For more information on MINS, refer to Anesthesia Updates on the NYSORA Anesthesia Assistant App. Get access to step-by-step management algorithms, the latest research, and peer-reviewed insights—all in one place. Download the Anesthesia Assistant App today and experience the future of anesthesia education and decision-making.
Reference: Wittmann M, Dinc T, Kunsorg A, Marcucci M, Ruetzler K. Preventing, identifying and managing myocardial injury after non cardiac surgery – a narrative review. Curr Opin Anaesthesiol. 2025;38(1):17-24.