Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
AboutBlock at a Glance
Infiltration around the sensory branches that provide innervation to the knee joint (genicular nerves) before they enter the knee capsule.
- Indications: Chronic knee pain, total knee arthroplasty, or procedures associated with moderate to severe postoperative knee pain
- Goal: Local anesthetic spread next to the genicular arteries (if visible) or at the junction of the epiphysis and diaphysis of the femur and tibia
- Local anesthetic volume: 4 to 5 mL per nerve
General Considerations
The genicular nerve block and radiofrequency ablation therapy were initially described to treat severe chronic pain of the knee. An extended version of the block technique under ultrasound (US) guidance was recently introduced to provide analgesia after knee surgery. The infiltration targets only the sensory branches to the knee joint, preserving quadriceps muscle strength. Thus, this novel analgesic technique could be used as an alternative when the femoral nerve and adductor canal blocks are not indicated or not desirable.
The first reported block of genicular nerves under fluoroscopy guidance was based on bony landmarks. The introduction of US allows for easy recognition of the same landmarks and provides additional visualization of the soft tissues and vessels needed to identify the injection site. The available data is still limited; however, case series show promising results of genicular nerve block in the perioperative setting. Clinical trials are currently ongoing to determine the efficacy of this novel technique to treat acute pain after total knee replacement.
Limitations
The genicular nerves vary in number and trajectory and, because of their small size, they are not visualized with the available US technology. Genicular nerve blocks are based on US landmarks, which may result in inconsistent analgesia, particularly if a low volume of local anesthetic (LA) is used.
Specific Risks
The proximity of the inferolateral genicular nerve (ILGN) to the common peroneal nerve (CPN) is a risk factor for unintended CPN block resulting in foot drop. Thus this nerve is spared if denervation is planned to treat chronic pain. Vascular or intraarticular punctures are other potential risks.
Anatomy
The innervation of the knee is complex, with branches originating from femoral, obturator, and sciatic nerves (Figure 1). The interindividual variability explains the discrepancy in the literature over the nomenclature and the origin of the genicular nerves.
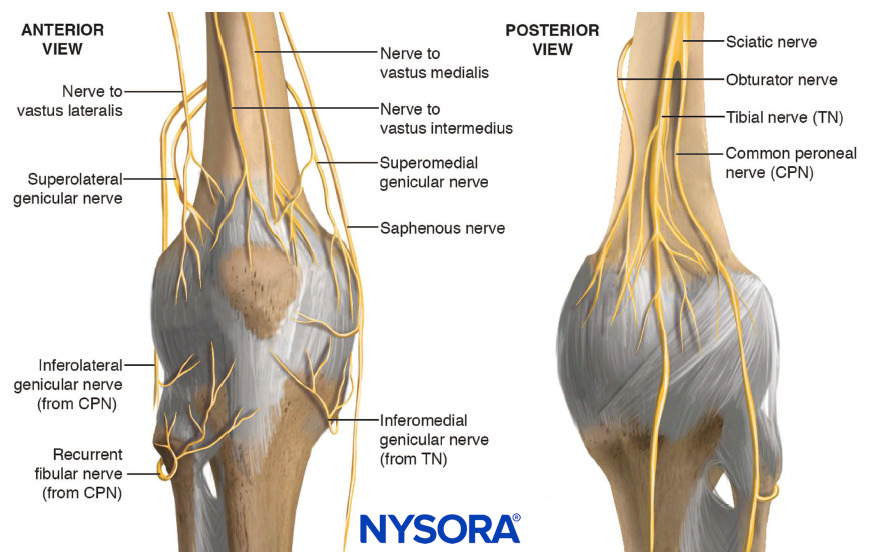
FIGURE 1. Innervation of the knee. The origin of the superomedial and superolateral genicular nerves (from the sciatic nerve or from the femoral nerve) is controversial.
To facilitate understanding of knee innervation, most authors divide the knee into an anterior and posterior compartment, and then further divide the anterior compartment into four quadrants. For the purpose of the technique description, the genicular nerves are called the superolateral (SLGN), superomedial (SMGN), inferolateral (ILGN), and inferomedial (IMGN) genicular nerves, which innervate primarily each corresponding quadrant. Several cadaver studies also show a contribution from other branches such as the recurrent peroneal nerve, the nerve to the vastus medialis, intermediate, lateralis, and the infrapatellar branch.
- The SLGN courses around the femur shaft to pass between the vastus lateralis and the lateral epicondyle. It accompanies the superior lateral genicular artery.
- The SMGN courses around the femur shaft, following the superior medial genicular artery, to pass between the adductor magnus tendon and the medial epicondyle below the vastus medialis.
- The ILGN courses around the tibial lateral epicondyle deep to the lateral collateral ligament, following the inferior lateral genicular artery, superior of the fibula head.
- The IMGN courses horizontally below the medial collateral ligament between the tibial medial epicondyle and the insertion of the collateral ligament. It accompanies the inferior medial genicular artery.
- The recurrent peroneal nerve originates in the inferior popliteal region from the common peroneal nerve and courses horizontally around the fibula to pass just inferior of the fibula head and travel superior to the anterolateral tibial epicondyle. It accompanies the recurrent tibial artery.
Ultrasound View
The relative position of the genicular nerves to bony landmarks at the level of the knee seems to be consistent according to the studies performed in cadavers, providing a reliable anatomic basis for an ultrasound-guided block. The US landmarks are the osteomuscular planes at the level of the metaphysis (the junction between the epiphysis and diaphysis) of the femur and tibia. Additional landmarks are the corresponding arteries, which follow the same path as the nerves and the collateral ligaments (Figure 2).
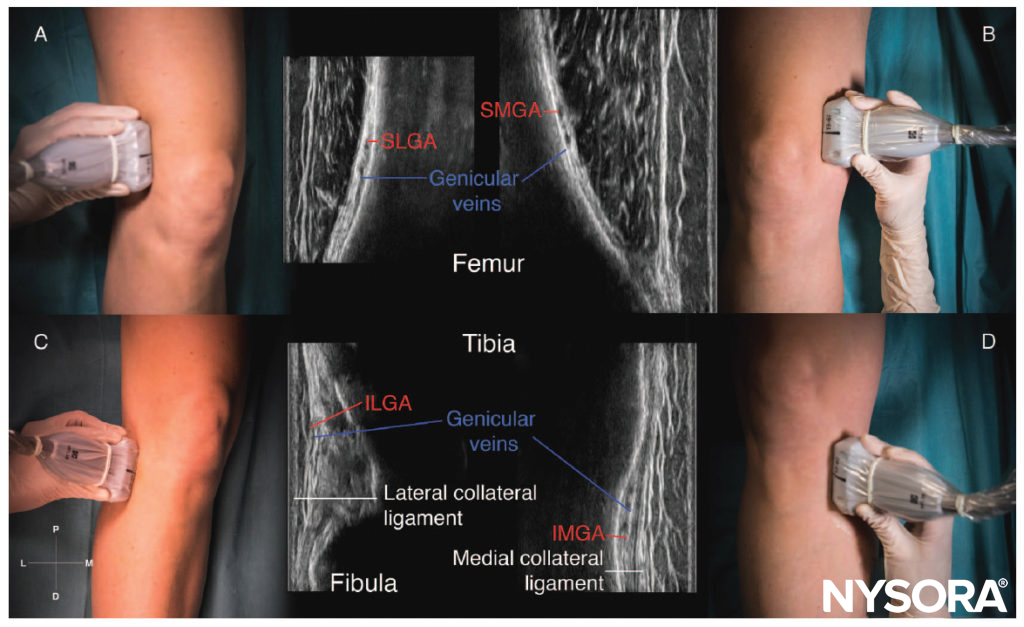
FIGURE 2. Sonoanatomy of the genicular nerves in a coronal plane. SLGA, superolateral genicular artery; SMGA, superomedial genicular artery; ILGA, inferolateral genicular artery; IMGA, inferomedial genicular artery. (A) Transducer position and sonoanatomy of the superomedial genicular nerve. (B) Transducer position and sonoanatomy of the inferomedial genicular nerve. (C) Transducer position and sonoanatomy of the superolateral genicular nerve. (D) Transducer position and sonoanatomy of the inferolateral genicular nerve.
Distribution of Analgesia
The genicular nerve block is a motor-sparing technique that anesthetizes the sensory terminal branches innervating the knee joint, resulting in anesthesia of the anterior compartment of the knee. The distribution of anesthesia of each nerve is mostly in the corresponding quadrant.
Block Preparation
Equipment
- Transducer: High-frequency, linear transducer
- Needle: 50-mm, 22-gauge, short-bevel needle
Learn more about Equipment for Regional Anesthesia.
Local Anesthetic
Long-lasting LAs such as bupivacaine or ropivacaine (0.25-0.5%) in a volume of 4 to 5 mL per nerve are suggested.
Patient Positioning
The patient is placed in a supine position with the knee slightly flexed by placing a pillow in the popliteal fossa (Figure 3).
FIGURE 3. Patient position to perform a genicular nerve block.
Technique
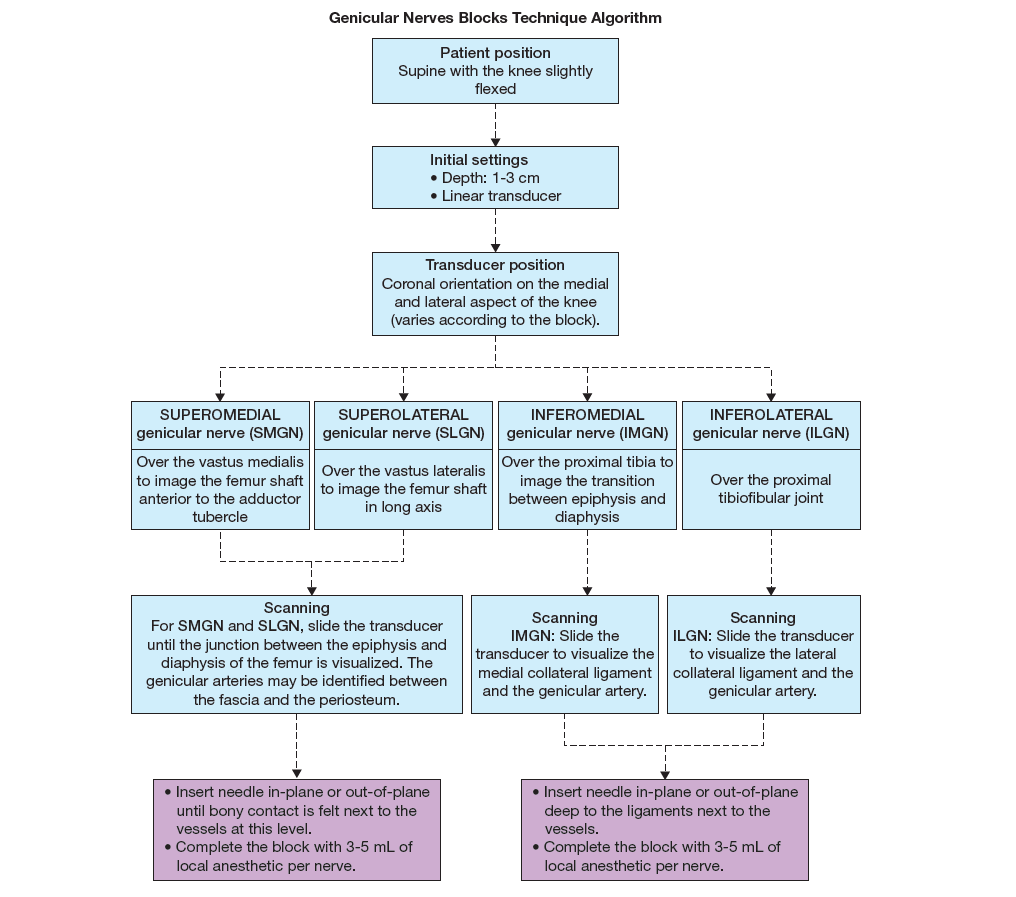
Initial Transducer Position and Scanning Technique
- SLGN: The transducer is placed in a coronal orientation over the lateral epicondyle of the femur and then moved proximally to visualize the metaphysis of the bone. The superolateral genicular artery may be seen between the deep fascia of the vastus lateralis and the femur at this level (see Figure 30-2A).
- SMGN: The transducer is placed in a coronal orientation over the medial epicondyle of the femur (see Figure 30-2B). The transducer is moved slightly proximally to visualize the metaphysis of the bone just anterior to the adductor tubercle. The SMG artery may be seen at this level between the deep fascia of the vastus medialis and the femur.
- ILGN: The transducer is placed in a coronal orientation over the lateral side of the distal knee. After identifying the lateral epicondyle of the tibia, the transducer is moved distally to visualize the head of the fibula. The inferolateral genicular artery may be seen between the collateral ligament and the lateral condyle of the tibia (see Figure 2C).
- IMGN: The transducer is placed in a coronal orientation over the medial condyle of the tibia and moved distally to visualize the metaphysis of the bone. At this level, the inferomedial genicular artery is seen beneath the medial collateral ligament (see Figure 2D).
- Additionally, the recurrent peroneal nerve can also be blocked: the transducer is placed in a coronal orientation over the anterolateral side of the distal knee to visualize the junction of the tibial lateral epiphysis and diaphysis, anterior of the fibula. The recurrent tibial artery is visualized superficial to the bone.
Needle Approach and Trajectory
Once the injection site has been identified, the needle tip is advanced next to the vessel (if seen) until bony contact is felt using an in-plane or out-of-plane approach. Alternatively, the transducer can be rotated in a transverse orientation and the needle tip redirected toward the bone surface. After confirming the correct position, the rest of the LA is injected (Figure 4).
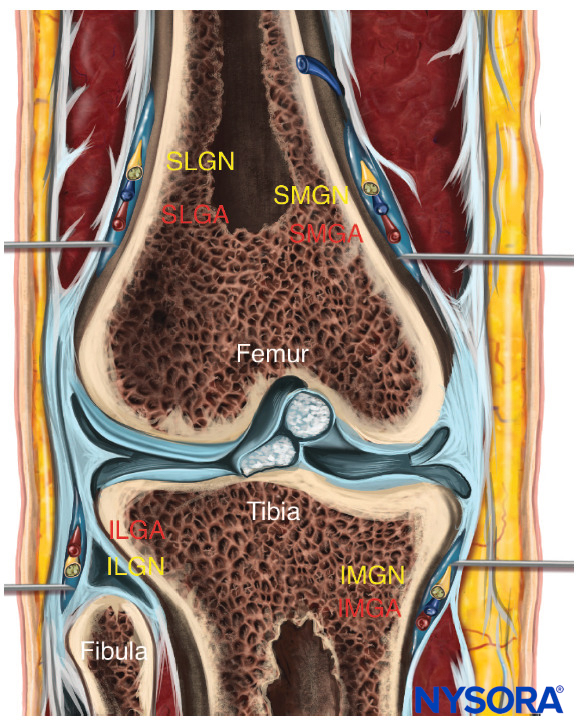
FIGURE 4. Reverse ultrasound anatomy of the genicular nerves showing needle insertion and distribution of the local anesthetic. SLGN, superolateral genicular nerve, and artery; SMGN, superomedial genicular nerve, and artery; ILGN, inferolateral genicular nerve, and artery; IMGN, inferomedial genicular nerve, and artery.
Flowchart
Clinical updates
Belba et al. (Regional Anesthesia & Pain Medicine, 2025) report 12-month and economic results from the COCOGEN pilot RCT comparing cooled vs conventional genicular RF for chronic knee pain (OA or persistent postsurgical pain after TKA) and found similar long-term responder rates (≥50% pain reduction) at 12 months. Notably, in the PPSP subgroup, cooled RF showed a significant advantage in mean NRS at 12 months (p=0.02) and appeared cost-saving with improved QALYs versus conventional RF—an effect not seen in OA.
- Read more about the study HERE.
Ferreira-Silva et al. (Regional Anesthesia & Pain Medicine, 2025) provide a critical appraisal of controversies in genicular nerve radiofrequency ablation (RFA) for knee osteoarthritis, highlighting that variability in outcomes likely reflects heterogeneity in patient selection and technical protocols. The authors conclude that prognostic blocks should be individualized (recommended in low pretest probability or post-TKA pain), that classical fluoroscopic landmarks may miss key branches of the SMGN/SLGN (supporting bipolar or expanded lesion strategies), and that three-nerve protocols may be insufficient given the anterior capsule’s ~10 articular nerve inputs—advocating compartment-based, personalized denervation (e.g., adding NVI, NVM/NVL, or RFN depending on OA distribution).
- Read more about the study HERE.
White et al. (British Journal of Anaesthesia, 2025) review motor-sparing regional anesthesia for total knee arthroplasty (TKA), concluding that adductor canal block (ACB), femoral triangle block, genicular nerve blocks, and iPACK—combined with surgical local infiltration analgesia (LIA)—optimize analgesia while preserving quadriceps strength and facilitating early mobilization. Evidence supports ACB over femoral nerve block for motor preservation with equivalent analgesia, with continuous ACB extending benefit beyond 24 hours in selected patients. LIA remains a practical benchmark but requires caution with high-dose ropivacaine due to variable peak plasma levels and a rare risk of LAST, particularly in older or low-weight patients.
- Read more about the study HERE.
de la Fuente-Escudero et al. (Pain Physician, 2026) conducted a randomized placebo-controlled trial showing that ultrasound-guided genicular nerve blocks (GNBs) with bupivacaine alone produced sustained reductions in knee osteoarthritis pain and improved WOMAC function scores through 24 weeks, with efficacy comparable to or better than bupivacaine plus triamcinolone. The addition of corticosteroids did not improve pain, function, stiffness, mood, or analgesic reduction outcomes, and the authors conclude that local anesthetic alone may be the safer and sufficient option for GNB treatment of knee OA.
- Read more about this HERE.