Dr. Hadzic will discuss the differences among the: (1) lumbar plexus block, (2) fascia iliaca block, (3) femoral triangle block, and (4) adductor canal block, because trainees and attendees to NYSORA workshops sometimes tend to be completely confused as to what each one of these blocks does.
The lumbar plexus derives its branches or origins from the spinal segments of L1 through L5 and is a rather large entity. But, in essence, the most important three nerves are the femoral nerve, which is the biggest nerve of the lumbar plexus, the lateral femoral cutaneous nerve of the thigh, and the obturator nerve.

Dr. Hadzic demonstrates the three nerves important for lumbar plexus block for the lower extremity, which are: femoral, lateral femoral cutaneous, and the obturator nerve.
If you open the abdominal cavity and dissect the source muscle then this is the image that you are going to see. These are the roots of the lumbar plexus, and these roots combine inside the source muscle in order to create the lumbar plexus.

Dr. Hadzic showing the roots of the lumbar plexus.
So when we perform a lumbar plexus block, it is here that the local anesthetic injection takes place, and we want to fill this space with the local anesthetic in order to get a block of all of those three nerves that we just talked about.

Dr. Hadzic demonstrates where the local anesthetic should be administered to block all three nerves.
One other way you can accomplish the lumbar plexus black is through the fascia iliaca by injecting the local anesthetic underneath the fascia iliaca, above the inguinal ligament which causes the local anesthetic to spread underneath the fascia iliaca and results in the block in most of these branches, particularly the femoral nerve.

Dr. Hadzic explains the alternative approach to the lumbar plexus block through the fascia iliaca.
If you take a look at the illustration on the left that mimics the aforementioned situation, you can see how the femoral nerve, lateral femoral cutaneous nerve of the thigh, and the obturator nerve are all covered by the fascia iliaca. So, the goal of the fascia iliaca block is actually an injection of the local anesthetic underneath the fascia iliaca in order to get the block of all of these nerves, but again, the main nerve that is blocked here is the femoral nerve.

Dr. Hadzic explains the alternative approach to the lumbar plexus block through the fascia iliaca.
And here’s how that works; shown below on the far right is the anatomy that we just reviewed with all the three main branches of the lumbar plexus. Also shown is the injection of the methylene blue underneath the fascia iliaca, and you can see the blue dye or methylene blue substantial distribution underneath the fascia iliaca to block these three branches of the lumbar plexus (femoral, lateral femoral cutaneous, and the obturator nerve).

The injection of the methylene blue underneath the fascia iliaca.
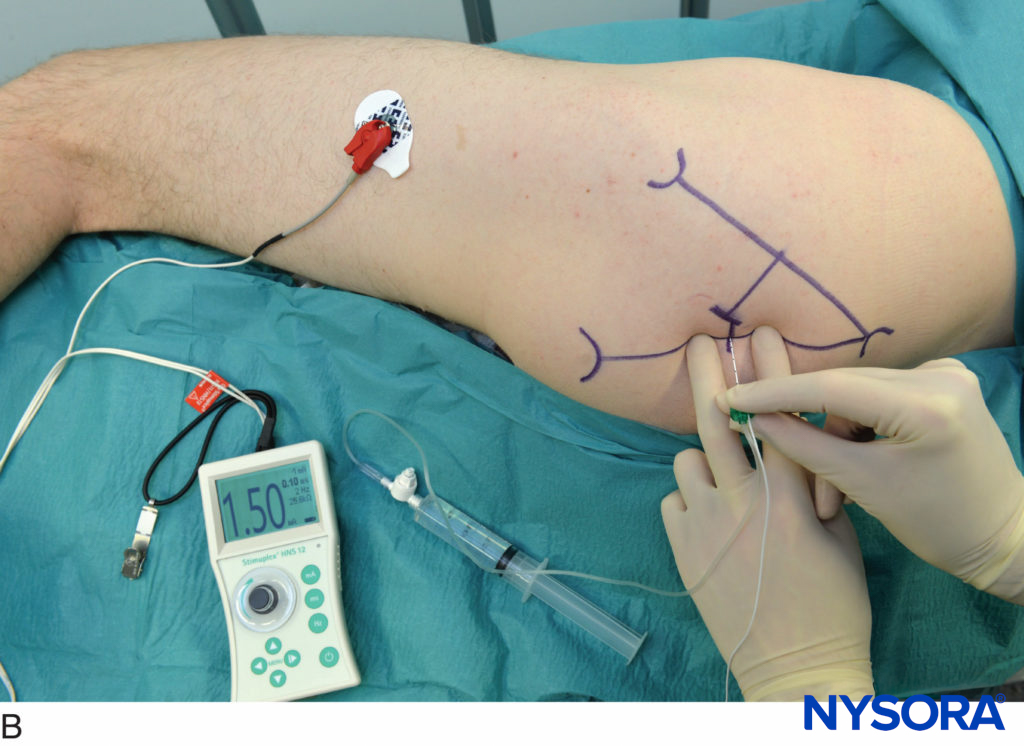
So far we talked about lumbar plexus, we talked about facilia iliaca as another approach to lumbar plexus block, but now once we are around the inguinal ligament, slightly above or below, we are talking about the femoral nerve. The femoral nerve occurs anywhere close to the inguinal ligament, and the idea with the femoral nerve is to deposit the local anesthetic around the femoral nerve in order to cause the block of all components of the femoral nerve.

Femoral nerve below the inguinal ligament.
But what is important to understand is that the femoral nerve can be blocked even inside the pelvis. It can be blocked around the inguinal ligament, and it can be blocked below the inguinal ligament. So the question really is, where does the femoral nerve block begin and end? As far as Dr. Hadzic is concerned, the femoral nerve block is a block of the femoral nerve anywhere it occurs – from the inside the pelvis, underneath the fascia iliaca, all the way down to the adductor canal.

Different block sites as the femoral nerve can be blocked anywhere on its path.
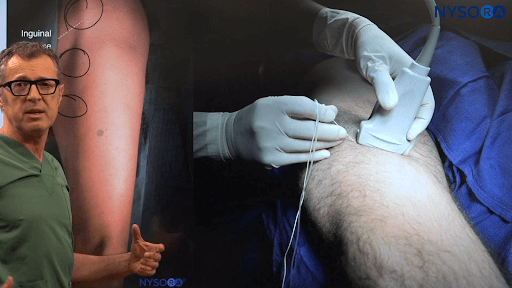
We have the inguinal ligament, the femoral artery and the femoral vein, and the femoral nerve is located lateral to the artery in its own sheath, and it’s underneath the fascia iliaca. But, these are all components of the femoral nerve that will travel distally, and as they travel distally the nerves give off branches to the different muscles, until they eventually end up in the adductor canal, as what remains of the femoral nerve, which is usually branches of the vastus medialis and esophagus nerve.

Different block sites as the femoral nerve can be blocked anywhere on its path.
So to recap, basically, if you do your injection around the inguinal ligament then you have a femoral nerve block. If you descend a little bit lower down then you have the femoral triangle block. And if you descend further down it’s the adductor canal block. But in all three instances what we are really blocking is elements of the femoral nerve.

Variants of the femoral nerve block, from proximal to distal.
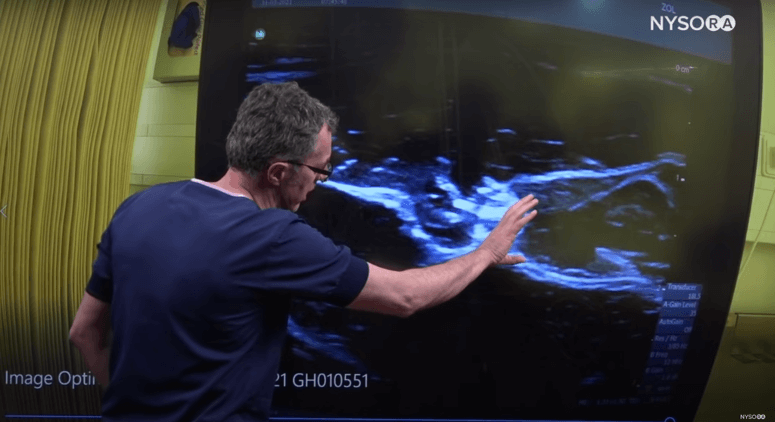
Below we can see the technique of the adductor canal block. Shown is the position to obtain adequate images, and you can see the sartorius muscle. Underneath the sartorius muscle is the femoral artery and the femoral vein, and the adductor longus muscle. But the femoral nerve or remains of the femoral nerve, such as the saphenous nerve and the nerve to the vastus medialis, are underneath the sartorius fascia in the triangle between the sartorius, vastus medialis muscle, and adductor longus muscle.

Dr. Hadzic demonstrating the functional anatomy for the adductor canal block.
So the injection of the local anesthetic wants to occur in that triangle to fill the space with the local anesthetic for this version of the femoral nerve block, or what remains of the femoral nerve in the adductor canal.
So far we have talked about the femoral nerve block, the femoral triangle block, and the adductor canal block. But if we descend lower down to the knee, and shown below is a patient who is having ruptured patellar repair, here you can inject local anesthetic to anesthetize the tissue for the patellar repair and it could be used as an analgesic, or even complete anesthetic if you will.

Infiltrational analgesia for quadriceps tendon.
But again, what’s really interesting is if you inject the local anesthetic around the knee for the quantitative standard repair, what we are really doing is blocking the terminal branches of the femoral nerve, because the anesthesia for this operation can be accomplished in any one of these locations, including the fascia iliaca and the lumbar plexus. Of course, the more distal you go, the more specific you will be. The choice of technique here usually being femoral nerve block, because it also causes relaxation of the quadriceps muscle, which then facilitates repair of the quadriceps tendon.
In summary, what we discussed is that the femoral nerve is a continuation of the same nerve from the pelvis all the way down to its terminal branches at the knee, and you have a chance to block it in various different locations alongside its path. While the femoral nerve gives off branches for the musculature proximally, it gives off branches for the sensory innervation more distally. Therefore, the more distal block of the femoral nerve that you perform, the more likely you are going to avoid the motor effect or motor weakness and promote ambulation, whereas the more proximal you do that, you’re going to get a great extent of analgesia, but at the same time you will get some motor weakness which may impair the ambulation.

Dr. Hadzic summarizes the different levels at which a femoral nerve block can be achieved.
So the choice at which level you want to do the femoral nerve block from here to there really depends on what you want to accomplish. The choice that you need to make is between the analgesia, which is best with the proximal approaches, and the modus pairing which is best with the distal approaches. Usually, a good compromise for the femoral nerve block for the total knee replacement in our practice is actually femoral triangle block, because the femoral triangle block will block most of the branches that we are interested in for total knee replacement pain management, but at the same time it spares the bulk of the muscles of the anterior thigh.
Watch the full video:
Clinical updates
Forero et al. (Current Anesthesiology Reports, 2025) synthesize the literature from 2013–2024 and conclude that regional anesthesia for total joint arthroplasty is inequitably delivered, with disparities linked to race/ethnicity and system-level factors such as hospital type and insurance status. They emphasize that evidence on the drivers of these gaps is sparse and—critically—there are no tested interventions shown to reduce these disparities, framing regional anesthesia utilization as a measurable anesthesia-quality equity target for future research.
Fathi et al. (BMC Anesthesiology, 2025) randomized 63 TKA patients (all under spinal anesthesia) to standard analgesia, genicular nerve block (GNB), or GNB + IPACK, and found the combination group had the lowest VAS pain scores at most timepoints (rest and movement) and the longest time to first rescue morphine. Total 24-h morphine use was also lowest with GNB+IPACK , and early functional recovery measures favored the combination strategy.
Belba et al. (Regional Anesthesia & Pain Medicine, 2025) report 12-month and economic results from the COCOGEN pilot RCT comparing cooled vs conventional genicular RF for chronic knee pain (OA or persistent postsurgical pain after TKA) and found similar long-term responder rates (≥50% pain reduction) at 12 months. Notably, in the PPSP subgroup, cooled RF showed a significant advantage in mean NRS at 12 months (p=0.02) and appeared cost-saving with improved QALYs versus conventional RF—an effect not seen in OA.
- Read more about the study HERE.
Gleicher et al. (Regional Anesthesia & Pain Medicine, 2025) in a double-blind placebo-controlled RCT (n=60) of outpatient/short-stay TKA, found that outpatient continuous adductor canal block (CACB) (0.2% ropivacaine infusion 5 mL/h × 60 h) produced markedly better recovery than single-shot ACB. CACB also reduced pain (rest and movement) and opioid consumption across the first 72 hours, with no major complications or LAST reported, supporting CACB to prevent rebound pain in fast-track pathways.
- Read more about the study HERE.
Illescas et al. (Regional Anesthesia & Pain Medicine, 2025) analyzed Premier database THA/TKA cases (2006–2021) and reaffirmed that neuraxial (vs general) anesthesia is associated with lower odds of multiple in-hospital adverse outcomes across both earlier (2006–2015) and more recent (2016–2021) eras, with some protective estimates stronger in 2016–2021 (e.g., acute renal failure and transfusion). Neuraxial use increased substantially over time (THA 10.7% in 2006 to 25.7% in 2021; similar for TKA), yet general anesthesia remained the most common, underscoring ongoing implementation gaps despite persistent outcome advantages.
- Read more about the study HERE.