Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Manage patients with chronic obstructive pulmonary disease (COPD) in the pre-, and perioperative period
Definition
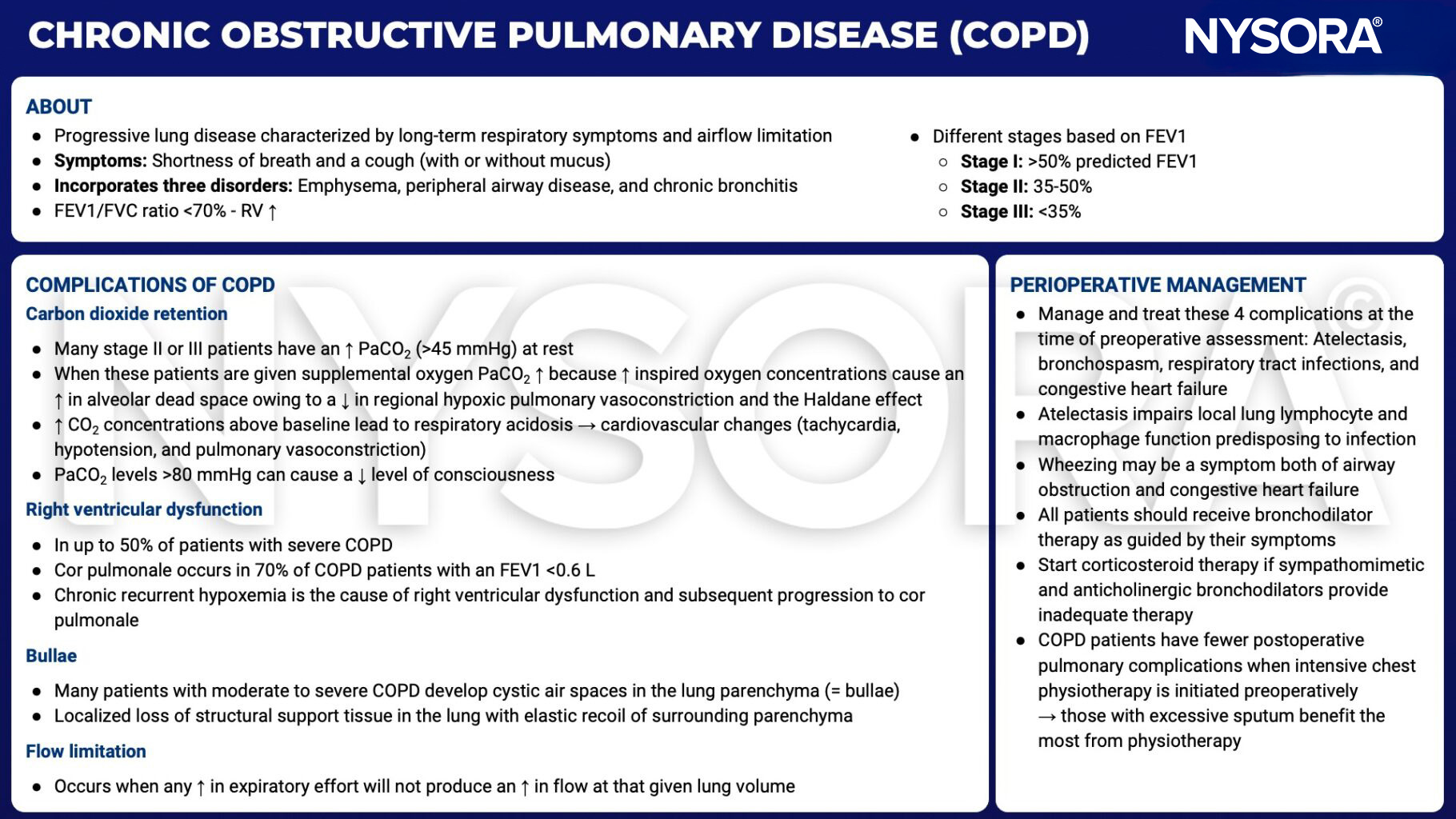
- COPD is an inflammatory lung disease characterized by abnormalities of the airways (bronchitis, bronchiolitis) and alveoli (emphysema), causing chronic dyspnea, cough, excessive sputum production, and progressive airway obstruction
Background information
- In 2017, 300 million people worldwide were living with COPD
Risk factors
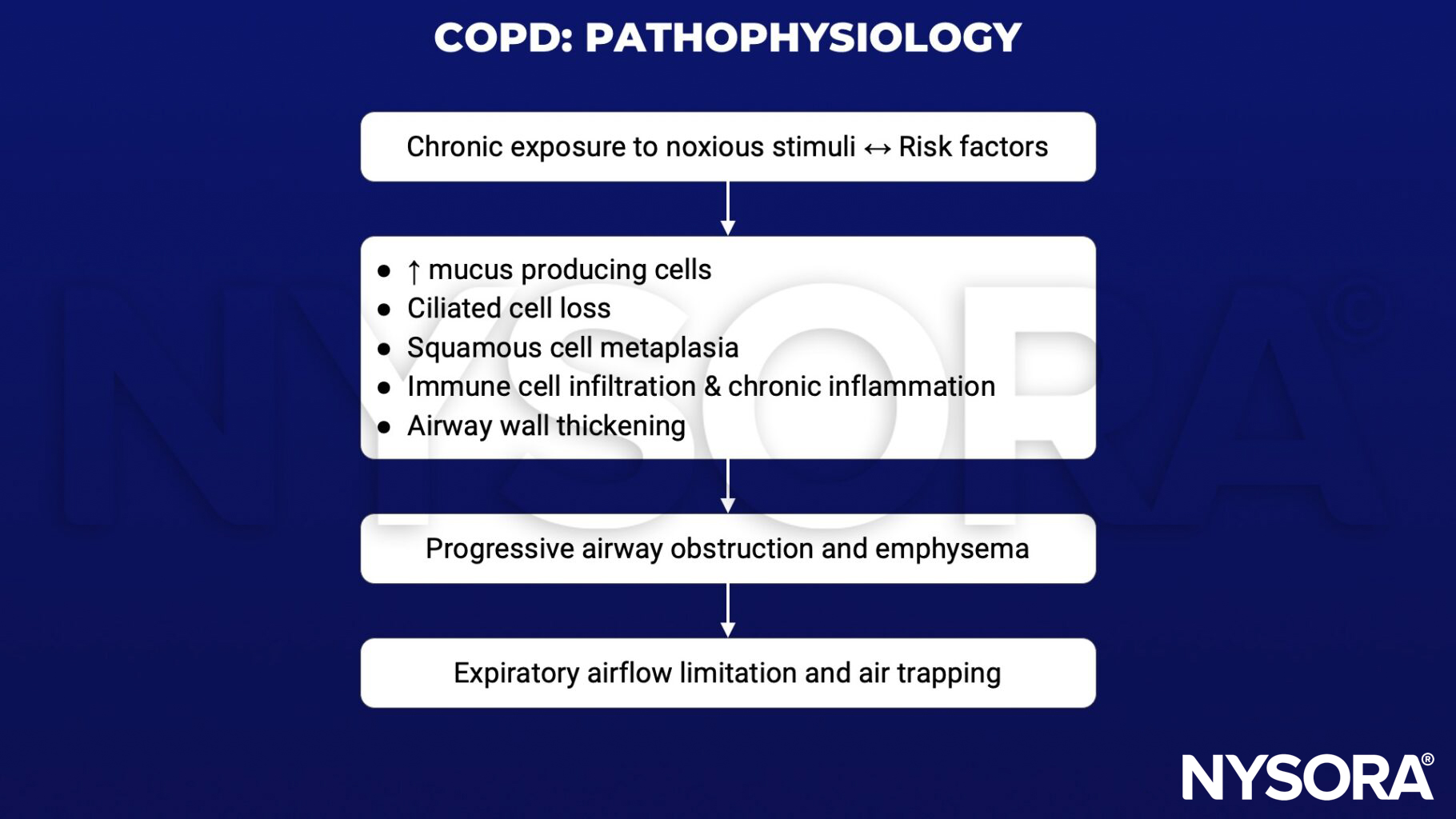
COPD is caused by a complicated interaction between chronic exposure to noxious stimuli, individual risk factors, and socioeconomic risk factors
Noxious stimuli
- Tobacco smoke
- Air pollution caused by burning carbon-based fuels or biomass
- Occupational exposure such as chemical fumes or other fine particulate matter
Individual risk factors
- History of previous lung infections, including tuberculosis
- Genetics
- Maternal and prenatal exposure
- Asthma
- Premature birth
Socio-economic risk factors
- Access to healthcare
- Diet
Pathophysiology
Exacerbation treatment
1. Assess severity
Use ABCDE approach – take arterial blood gas, perform chest X-ray, apply full ASA-monitoring
2. Treat symptoms
- Give supplemental O2 – titrate to achieve SaO2 of 88-92%
- Bronchodilators
- ↑ dose and/or frequency of short-acting bronchodilators
- Combine short-acting beta-2-agonists and anticholinergics
- Give long-acting beta-2-agonists when stable
- Give corticosteroids
- Give antibiotics if signs of bacterial infection
- If necessary, start noninvasive ventilation (NIV)
3. Identify and treat associated conditions
e.g., Heart failure, pulmonary embolism, arrhythmia
Anesthetic implications
Preoperative assessment
- Assess maximal level of exertion attainable
- Perform
- Routine preoperative blood tests
- Electrocardiogram – to exclude concomitant heart disease
- Chest X-ray – if evidence of current infection or recent worsening of symptoms
- Spirometry – to confirm the diagnosis and to assess the severity of COPD
- Treat symptoms aggressively
- If signs of active respiratory infection, postpone non-emergency surgery
- Strict smoking cessation
- Preoperative physiotherapy may help reduce the incidence of intraoperative bronchial plugging or pneumonitis
- Optimize nutritional status
- Obesity and underweight both increase perioperative risk
- Serum albumin level <35 mg/L is a strong predictor of postoperative pulmonary complications, give preoperative nutritional supplementation
Anesthetic regimen
- Regional anesthesia (RA) decreases postoperative pulmonary complications
- Light sedation, flexible positioning, or NIV might comfort patients who find it uncomfortable lying supine
- General anesthesia in COPD carries higher risk for laryngospasm, bronchospasm, cardiovascular instability, barotraumas, and hypoxemia
- To reduce the harmful effects of air trapping when mechanically ventilating
- Reduce the respiratory rate or the I:E ratio (to 1:3–1:5) to lengthen expiration
- Give PEEP to help keep small airways open during late exhalation
- Promptly treat bronchospasm
- Fully reverse the neuromuscular blocking agent before extubation
- Consider peri-extubation bronchodilator treatment
- NIV post-extubation reduces the work of breathing and air trapping and has been shown to reduce the need for reintubation in the postoperative period after major surgery
Suggested reading
- Christenson SA, Smith BM, Bafadhel M, Putcha N. Chronic obstructive pulmonary disease. Lancet. 2022;399(10342):2227-2242.
- National Institute for Health and Care Excellence. (2018) Chronic Obstructive Pulmonary Disease in over 16s: diagnosis and management (NICE guideline 115) available at https://www.nice.org.uk/guidance/ng115.
- Lumb AB, Biercamp C. Chronic obstructive pulmonary disease and anaesthesia. Continuing Education in Anaesthesia, Critical Care & Pain. 2014;14:1-5.
Clinical updates
Cohen E (Current Opinion in Anesthesiology, 2025) outlines emerging regenerative strategies for end-stage COPD, highlighting that alveolar epithelial progenitor (AEP) cells and AECII stem-cell–mediated regeneration may restore damaged alveolar–capillary units rather than merely slow decline. The review details advances in 3D lung organoids and whole-lung bioengineering using decellularized scaffolds repopulated with autologous or induced pluripotent stem cells within bioreactors to recreate functional gas-exchange surfaces. Although currently limited to preclinical models, these technologies aim to provide immunocompatible, transplantable lung tissue, potentially offering a future alternative to donor-dependent lung transplantation for advanced COPD.