
 Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Describe the mechanism and risk factors of laryngospasm
- Prevent laryngospasm
- Recognize and treat laryngospasm
Background
- Laryngospasm is the sustained closure of the vocal cords resulting in partial or complete loss of the airway
- Primitive protective airway reflex to prevent tracheobronchial aspiration after an offending stimulus
- Problematic prolongation of this initial reflex can occur under general anesthesia, often during intubation or extubation
- Can rapidly result in hypoxemia and bradycardia
- Overall incidence ~1%
- Incidence up to 25% in patients undergoing tonsillectomy and adenoidectomy
Signs
- Respiratory stridor
- Paradoxical respiratory movements
- Suprasternal and supraclavicular retractions
- Rapidly decreasing oxygen saturation
- Excessive chest movements but no movement of the reservoir bag and no capnogram reading
- Bradycardia
- Negative pressure pulmonary edema
- Cardiac arrest
- Pulmonary aspiration
- Arrhythmias
Risk factors
| Patient-related | Surgery-related | Anesthesia-related |
|---|---|---|
| Obesity | Nasal, oral or pharyngeal surgeries (adenoidectomy and tonsillectomy) | Laryngeal mask/Guedel airway device |
| Young age | Gastrointestinal endoscopy | Extubation |
| Active and passive smoking | Bronchoscopy | Suction catheter |
| ASA IV | Appendectomy | Light anesthesia plan |
| Gastroesophageal reflux | Anal or cervical dilatation | Blood/secretions in the airway |
| Obstructive sleep apnea | Mediastinoscopy | Regurgitation |
| Upper airway infection | Inferior urologic surgery | Desflurane |
| Hypocalcemia | Skin transplant | Ketamine and thiopental induction |
| Asthma | Nociception | Nasogastric tube |
| Difficult airway | Surgical stimulus | Inexperience of anesthesiologist |
| Movement | Failed intubation | |
| Recurrent laryngeal nerve damage | Laryngoscopy | |
| Esophageal stimulation | ||
| Iatrogrnic removal of parathyroid glands |
Prevention
- Anesthetic technique
- Ensure adequate depth
- Inhalation induction with non-irritant agent (e.g., sevoflurane)
- IV induction with propofol is less problematic
- Extubate either in a deep plane of anesthesia or fully awake, but not in-between
- “Deep” extubation: Suction the airway and place the patient in a lateral position
- Awake extubation: Once facial grimacing, adequate tidal volume, a regular respiratory pattern, coughing, and preferably eye opening have returned, use “no touch” technique: Pharyngeal suctioning and lateral positioning while anesthetized, followed by avoidance of any stimulation until eye opening when extubation is performed
- Extubation during forced positive pressure inflation decreases laryngeal adductor excitability, decreasing the risk of laryngospasm
- Pharmacological prevention
- Magnesium 15 mg/kg IV intraoperatively
- Lidocaine topically 4 mg/kg or IV 1.5-2 mg/kg (further research needed)
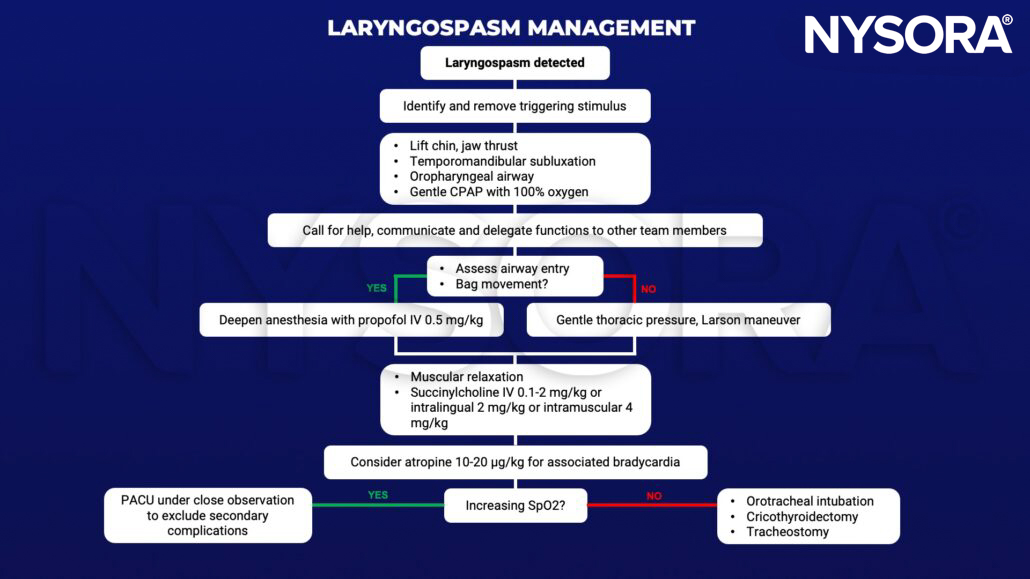
Management
Suggested reading
- Gavel G, Walker RWM. Laryngospasm in anaesthesia. Continuing Education in Anaesthesia Critical Care & Pain. 2014;14(2):47-51.
- Silva CR, Pereira T, Henriques D, Lanca F. Comprehensive review of laryngospasm. WFSA Resource Library. https://resources.wfsahq.org/uia/volume-35/comprehensive-review-of-laryngospasm/. Published July 8, 2020. Accessed February 2, 2023.
- Visvanathan T, Kluger MT, Webb RK, Westhorpe RN. Crisis management during anaesthesia: laryngospasm. Qual Saf Health Care. 2005;14(3):e3.
Clinical updates
Disma et al. (British Journal of Anaesthesia, 2024) published the first joint ESAIC–BJA guidelines dedicated to airway management in neonates and infants, emphasizing strategies to reduce airway complications such as laryngospasm. Key recommendations include ensuring adequate anesthetic depth, routine use of neuromuscular blockade when appropriate, limiting intubation attempts, and favoring awake extubation in high-risk patients.
- Read more about this study HERE.
Stepanovic et al. (British Journal of Anaesthesia, 2024) report that children with current or recent upper respiratory tract infections have a 2–3-fold increased risk of perioperative respiratory adverse events, including laryngospasm. Higher risk is seen in children under 2 years and those with active symptoms, while use of supraglottic airway devices, total intravenous anesthesia with propofol, and appropriate case deferral significantly reduces complications. These findings reinforce URTI status as a key, modifiable risk factor for laryngospasm in pediatric anesthesia.
- Read more about this study HERE.
Kojima et al. (Anesthesiology, 2025) prospectively analyzed over 17,000 pediatric airway management encounters and found that airway adverse events, including laryngospasm, occurred in 1.1% of cases, with the highest risk in neonates, infants, and children with difficult airway features. Use of supraglottic airway devices and muscle relaxants at the first attempt was associated with a significantly lower incidence of respiratory complications.
- Read more about this study HERE.











