Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Recognize the signs and symptoms of bronchospasm
- Manage and prevent bronchospasm
Definition and mechanism
- Bronchospasm or a bronchial spasm is a sudden constriction of the muscles in the walls of the bronchioles
- It is caused by the release (degranulation) of substances from mast cells or basophils under the influence of anaphylatoxins
Signs and symptoms
- Wheezing
- Prolonged expiration
- ↑ Peak inspiratory pressure
- ↓ Exhaled tidal volume
- ↓ Oxygen saturation
- A delayed rise in end-tidal CO2 on capnograph
- Hypotension
- Moderate tachycardia
- ↑ Resistance
- ↓ Lung compliance
Causes
- Bronchospasm is a reversible reflex spasm of the smooth muscle in the bronchi and is vagally mediated and is more common in asthmatics
- Histamine, released due to stimuli such as cold air, smoking, upper respiratory tract infection, or inhaled irritants, provokes bronchospasm
- Bronchospasm during the perioperative period may be caused by anaphylaxis, tracheal intubation, drugs (i.e., morphine or atracurium)
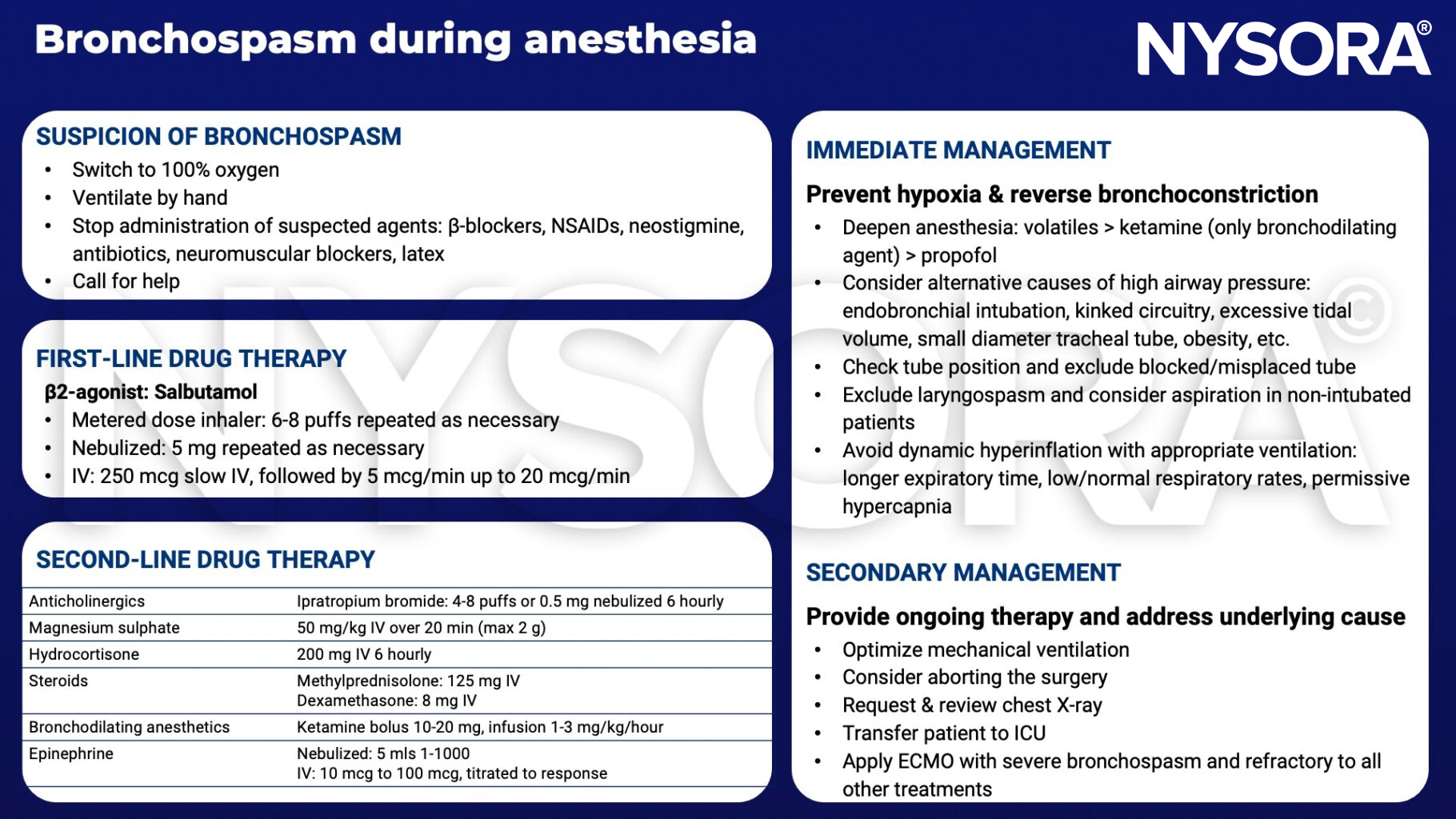
Management
Pre-operative management
- Supplemental oxygen
- Inhaled β2-agonists
- Intravenous steroids
Intra-operative management
Prevention
- Perform a thorough assessment of the patient before surgery
- Careful medication history should be taken with particular reference to drug sensitivities
- Encourage the patient to stop smoking preoperatively
- Wheezing, cough increased sputum production, shortness of breath and diurnal variability in peak expiratory flow rate (PEFR) indicate poor control
- Recent or frequent exacerbations or admission to the hospital may be an indication to postpone non-essential surgery
Keep in mind
The risk of bronchospasm is reduced by:
- Pretreatment with an inhaled/nebulized beta-agonist, 30 minutes prior to surgery
- Induction of anesthesia with propofol
- An adequate depth of anesthesia before airway instrumentation
Suggested reading
- Pollard BJ, Kitchen, G. Handbook of Clinical Anaesthesia. Fourth Edition. CRC Press. 2018. 978-1-4987-6289-2.
- Vojdani S. Bronchospasm During Induction of Anesthesia: A Case Report and Literature Review. Galen Med J. 2018 May 19;7:e846.
- Pascale Dewachter, Claudie Mouton-Faivre, Charles W. Emala, Sadek Beloucif, Bruno Riou; Case Scenario: Bronchospasm during Anesthetic Induction. Anesthesiology 2011; 114:1200
- Westhorpe RN, Ludbrook GL, Helps SC. Crisis management during anaesthesia: bronchospasm. Qual Saf Health Care. 2005;14(3):e7.
Clinical updates
Stepanovic et al. (British Journal of Anaesthesia, 2024) report that children with current or recent upper respiratory tract infection have a 2–3-fold increased risk of perioperative respiratory adverse events, including bronchospasm, laryngospasm, and desaturation, particularly in those < 2 years old or with asthma or recent infection. The authors recommend postponing elective surgery for at least 2 weeks, preferential use of supraglottic airway devices over tracheal tubes, TIVA with propofol, avoidance of desflurane, and consideration of preoperative salbutamol or dexmedetomidine to reduce bronchospasm risk. Risk stratification using tools such as the COLDs score is emphasized to guide perioperative decision-making and mitigate bronchospasm-related complications.
- Read more about this study HERE.
Kojima et al. (Anesthesiology, 2025) report in the prospective multicenter J-PEDIA study that airway-related adverse events occurred in 1.1% of cases, including bronchospasm, with overall airway complications in 2.0%. Neonates and infants were at the highest risk, particularly those with airway sensitivity or difficult airway features. First-attempt use of supraglottic devices and muscle relaxants was associated with reduced adverse events, suggesting that optimized intubation conditions and device selection may mitigate bronchospasm risk during pediatric airway management.
- Read more about this study HERE.
Savic et al. (Anesthesiology, 2025) review sugammadex-associated hypersensitivity reactions, highlighting that perioperative anaphylaxis may present with bronchospasm, hypotension, and cardiovascular collapse, often occurring immediately after reversal of neuromuscular blockade. The authors describe both IgE-mediated and non-IgE mechanisms, explaining reactions even on first exposure. Prompt recognition and treatment with epinephrine, oxygen, fluids, and antihistamines are emphasized, along with post-event allergy testing, underscoring that sugammadex-related bronchospasm should be considered in unexplained end-of-case respiratory compromise.
- Read more about this study HERE.