Learning objectives
- Definition of acute kidney injury (AKI)
- Pre- and perioperative management of AKI
Definition and mechanisms
- AKI is an acute decline (hours to days) in renal function leading to the retention of plasma urea and creatinine
- AKI leads to dysregulation of volume status, metabolic acidosis, and electrolytes
- Perioperative AKI:
- Occurs in approximately 1% of patients undergoing general surgery
- Is associated with an increased risk of sepsis, anemia, coagulopathy, and mechanical ventilation
Signs and symptoms
- ↑ Serum creatinine concentration
- ↑ Blood urea nitrogen concentration
- Patients are not necessarily oliguric
Classification and causes of AKI
- Pre-renal – inadequate perfusion – 40%–70%
- Renal – intrinsic renal disease – 10%–50%
- Post-renal – Obstructive uropathy – 10%
| Hemodynamic 'pre-renal' | Intrinsic renal disease | Post-renal |
|---|---|---|
| Hypovolemia: Bleeding Dehydration Extravasation | Acute tubular injury: Systemic inflammation Sepsis Major surgery Prolonged or total ischemia | Obstruction: Prostatic hypertrophy Nephrolithiasis Retroperitoneal fibrosis Pelvic masses Bladder tumors |
| Vasodilatory hypotension: Sepsis | Exogenous nephrotoxins: Aminoglycosides Radiological contrast | |
| Low cardiac output states | Pigment nephropathy; Rhabdomyolysis Hemolysis including cardiopulmonary bypass | |
| Acute and chronic heart failure | Metabolic syndromes: Hypercalcemia Hyperuricaemia | |
| Locally impaired renal circulation: Medication (ACEI, A2RB, NAIDS) Renovascular disease CKD Chronic liver disease abdominal compartment syndrome | Autoimmune/inflammatory: Glomerulonephritis Vasculitis Thrombotic microangiopathies Interstitial nephritis |
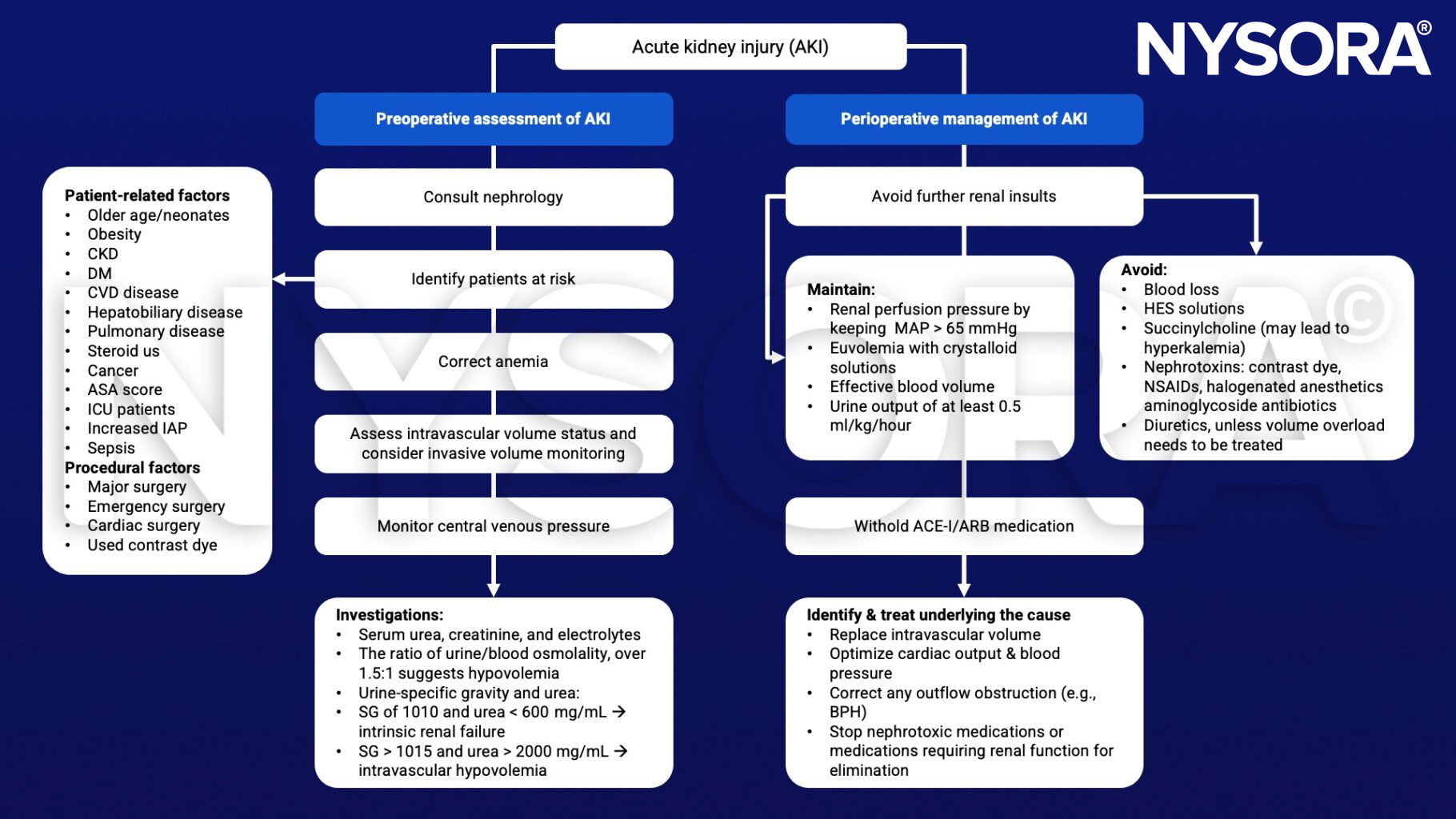
Management
Keep in mind
- Patients in whom chronic diuretic therapy has caused hypo– or hyperkalemia may have:
- Potentiation of the effects of muscle relaxant
- A predisposition to cardiac arrhythmias and acute kidney injury
Suggested reading
- Gumbert SD, Kork F, Jackson ML, et al. Perioperative Acute Kidney Injury. Anesthesiology. 2020;132(1):180-204.
- Pollard BJ, Kitchen, G. Handbook of Clinical Anaesthesia. Fourth Edition. CRC Press. 2018. 978-1-4987-6289-2.
- Goren O, Matot I. Perioperative acute kidney injury. Br J Anaesth. 2015;115 Suppl 2:ii3-ii14.
- Gross JL, Prowle JR. Perioperative acute kidney injury, BJA Education, Volume 15, Issue 4, 2015, Pages 213–218.
Clinical updates
Trocheris-Fumery et al. (Anesthesiology, 2025) demonstrated that early continuous norepinephrine infusion during anesthesia induction in high-risk patients undergoing major abdominal surgery significantly reduced postoperative complications compared with reactive ephedrine (44% vs 58%) and markedly decreased hypotensive episodes (15% vs 74%). Given the strong link between intraoperative hypotension and acute kidney injury (AKI), improved hemodynamic stability and lower lactate levels suggest that a proactive norepinephrine strategy may help reduce hypotension-related renal injury.
- Read more about this topic HERE.
Cheruku et al. (Anesthesiology, 2025) found that higher levels of C-terminal FGF23 in the blood just 6 hours after cardiac surgery were strongly linked to the development of acute kidney injury (AKI) during hospitalization. In 173 patients undergoing CABG and/or valve surgery, those with a two-fold rise in this biomarker had about a 60% higher risk of AKI, and the test predicted kidney injury earlier than serum creatinine. These findings suggest that measuring C-terminal FGF23 shortly after surgery could help clinicians identify high-risk patients sooner and start kidney-protective strategies earlier.
- Read more about this topic HERE.
Calabrese et al. (Anesthesiology, 2026) review how targeting the renin–angiotensin system (RAS) can personalize treatment for critically ill patients, especially those with vasodilatory shock, ARDS, and acute kidney injury (AKI). They highlight that angiotensin II infusion is most beneficial in patients with high renin levels, ACE inhibitor use, or severe AKI requiring renal replacement therapy, where it improves blood pressure and may improve survival in selected subgroups. The authors also emphasize restarting ACE inhibitors or ARBs after AKI to reduce long-term kidney damage and explore emerging therapies that activate the protective “alternative” RAS pathway.
- Read more about this topic HERE.