Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About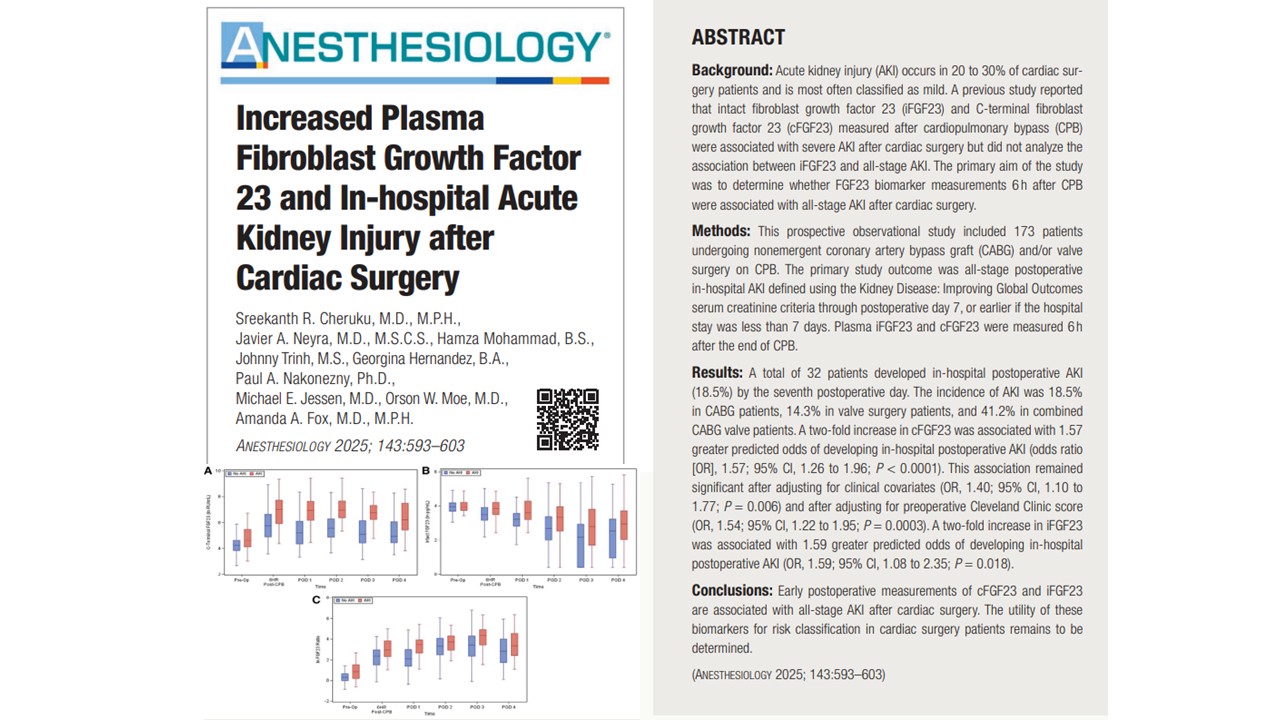

A new study published in Anesthesiology (September 2025) by Cheruku et al. offers promising news for clinicians seeking to detect acute kidney injury (AKI) earlier in patients undergoing cardiac surgery. Researchers at the University of Texas Southwestern Medical Center have found that plasma levels of fibroblast growth factor 23 (FGF23)—measured just six hours after cardiopulmonary bypass (CPB)—are significantly associated with the development of AKI during hospitalization.
This biomarker-based approach may pave the way for earlier risk stratification, more timely interventions, and ultimately better outcomes for a population that faces significant renal risk following heart procedures.
The persistent problem of AKI after cardiac surgery
Cardiac surgery is among the most common high-risk procedures worldwide, with over 2 million patients undergoing coronary artery bypass grafting (CABG) or valve surgery annually. One of the most concerning complications associated with these procedures is acute kidney injury, which develops in approximately 20% to 30% of patients. Even mild AKI is not benign; it is linked with significantly higher rates of mortality, morbidity, progression to chronic kidney disease (CKD), and increased hospital length of stay.
Despite its prevalence, the early detection of AKI remains a significant challenge. The current standard diagnostic criteria rely heavily on serum creatinine measurements and urine output, both of which are influenced by hemodilution, fluid shifts, and other perioperative factors. Moreover, serum creatinine levels typically rise only after kidney function has already deteriorated, making them a late-stage indicator rather than an early warning system.
This diagnostic lag opens a critical window of missed opportunity—where early intervention might prevent worsening of kidney damage. The search for better biomarkers has thus become a pressing area of research in perioperative and critical care medicine.
What is FGF23, and why is it important?
Fibroblast growth factor 23 (FGF23) is a hormone primarily secreted by bone-forming cells (osteoblasts and osteocytes). It plays a central role in phosphate regulation by acting on the kidneys to increase phosphate excretion and suppress vitamin D activation.
There are two principal forms of FGF23 measurable in blood:
- Intact FGF23 (iFGF23): The full-length, biologically active form of the protein.
- C-terminal FGF23 (cFGF23): This includes both the intact hormone and its cleaved C-terminal fragment.
These forms have distinct biological and clinical roles. While iFGF23 exerts direct hormonal effects, cFGF23 may act as a competitive antagonist and is often elevated in inflammatory and disease states. Prior research has shown that FGF23 levels increase in patients with declining kidney function and that they are independently associated with mortality in patients with end-stage renal disease.
The novel aspect of the current study is that it evaluates both cFGF23 and iFGF23 in the immediate postoperative setting, aiming to determine their association with all-stage AKI, rather than just severe cases.
Study design and methodology
This was a prospective observational study that included 173 patients undergoing nonemergent CABG and/or valve surgery on CPB. Conducted at a single academic center, the study was nested within a broader observational trial and utilized plasma samples stored in a biobank.
The researchers measured plasma levels of cFGF23 and iFGF23 exactly six hours after the end of CPB. This time point was strategically chosen because it precedes most clinical diagnoses of AKI and avoids the confounding effects of later postoperative changes. The primary outcome was in-hospital AKI, defined using KDIGO serum creatinine criteria.
Patient characteristics such as age, body mass index (BMI), estimated glomerular filtration rate (eGFR), CPB time, and pre-existing kidney disease were collected to control for potential confounders.
Key results
The findings were both statistically significant and clinically relevant. Among the 173 patients, 32 (18.5%) developed AKI by postoperative day 7. The breakdown showed that combined CABG and valve surgery carried the highest risk, with an AKI rate of 41.2%.
The researchers found that:
- A two-fold increase in cFGF23 levels at 6 hours post-CPB was associated with a 1.57-fold increase in the odds of developing AKI.
- This association remained statistically significant even after adjusting for key clinical variables and the Cleveland Clinic preoperative AKI risk score.
- Similarly, a two-fold increase in iFGF23 was associated with a 1.59-fold increase in AKI risk, but this was not significant after adjustment for covariates.
- The ratio of cFGF23 to iFGF23 was also associated with AKI, reinforcing the dominant role of cFGF23.
These results highlight cFGF23 as the most robust and consistent biomarker in predicting all-stage postoperative AKI.
Predictive accuracy
The predictive power of cFGF23, as measured by the area under the receiver operating characteristic curve (AUC), was 0.73 when unadjusted and 0.81 when adjusted for covariates—outperforming many previously studied biomarkers.
For context, here’s how FGF23 compares with other known AKI biomarkers:

These comparisons suggest that cFGF23 may represent one of the most accurate early biomarkers for all-stage AKI in the setting of cardiac surgery—especially when mild AKI is considered, which other biomarkers often fail to detect.
Clinical implications and future directions
The ability to identify AKI risk within hours after surgery creates a critical window for intervention. Patients with elevated cFGF23 could be targeted for:
- Enhanced hemodynamic monitoring
- Avoidance of nephrotoxins
- Implementation of the KDIGO AKI prevention bundle
- Use of amino acid infusions or goal-directed perfusion strategies has been shown to mitigate kidney injury
Moreover, integrating FGF23 measurements into clinical workflows—such as electronic health record alerts—could streamline the identification of at-risk patients and guide real-time clinical decision-making.
Further studies are needed to:
- Establish threshold values for clinical use
- Evaluate long-term outcomes such as CKD progression and mortality
- Investigate the role of α-klotho expression and its interaction with FGF23 in AKI pathophysiology
Limitations
While the findings are compelling, several limitations must be acknowledged. The study was conducted at a single center, which may limit its generalizability. It also lacked urine output data in its definition of AKI, relying solely on serum creatinine criteria.
Moreover, the sample size, though sufficient for primary analyses, may not be powered to detect subtle associations or differences in subgroup analyses—such as between different AKI stages or between iFGF23 and cFGF23 performance across surgical types.
Despite these limitations, the study provides a strong foundation for future multicenter trials.
Conclusion
The study presents compelling evidence that C-terminal FGF23, measured just 6 hours after cardiac surgery, serves as a powerful predictor of all-stage in-hospital AKI. Its performance rivals and may exceed that of current biomarker candidates, offering clinicians an earlier and more accurate method to identify at-risk patients.
As the field of perioperative medicine continues to evolve, integrating molecular biomarkers such as FGF23 into standard care protocols could revolutionize how we manage AKI—a condition that remains all too common and devastating in surgical populations. With additional research, FGF23 could become a mainstay in the toolkit of predictive medicine, allowing for earlier diagnosis, more personalized care, and improved patient outcomes after cardiac surgery.
To read more, refer to the full article in Anesthesiology.
Cheruku SR, Neyra JA, Mohammad H, Trinh J, Hernandez G, Nakonezny PA, Jessen ME, Moe OW, Fox AA. Increased Plasma Fibroblast Growth Factor 23 and In-hospital Acute Kidney Injury after Cardiac Surgery. Anesthesiology. 2025 Sep 1;143(3):593-603.
Read more about acute kidney injury in our Anesthesiology Module on NYSORA 360—a complete training resource designed for residents, with practical, up-to-date guidance on perioperative and critical care management.