
 Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Description of a uterine rupture
- Management of a uterine rupture
Definition and mechanisms
- Uterine rupture refers to a complete division of all three layers of the uterus: the endometrium (inner epithelial layer), myometrium (smooth muscle layer), and perimetrium (serosal outer surface)
- Typical rupture occurs during labor, but it may occasionally happen earlier in pregnancy
- The fetus is left without the protection of the uterus, leaving the fetus without oxygen and causing the fetus’s heart rate to slow down
- Suspect uterine rupture based on a rapid drop in the baby’s heart rate during labor
- The cardinal sign of uterine rupture is loss of fetal station on a manual vaginal exam
- The maternal mortality rate is < 1%, fetal mortality rate is between 2-6 %
- Incomplete rupture:
- Peritoneum is still intact
- Complete rupture:
- All three layers are ruptured
- The contents of the uterus spill into the peritoneal cavity or the broad ligament
- Bladder injury is not uncommon with uterine rupture
- A caesarean section is recommended in women who have had a prior rupture
Signs and symptoms
- Vaginal bleeding
- Abdominal pain and tenderness
- Chest pain, pain between the scapulae, or pain on inspiration
- Hypovolemic shock
- Signs associated with fetal oxygenation:
- Late deceleration
- Reduced variability
- Tachycardia
- Bradycardia
- Absent fetal heart sounds
- Cessation of uterine contractions
- Palpation of the fetus outside the uterus (usually occurs only with a large, complete rupture)
Risk factors
- History of uterine surgery
- Previous uterine rupture
- Uterine trauma
- Congenital uterine anomalies such as septate uterus or bicornuate uterus
- Vaginal birth after caesarean section
- Trauma
- Cocaine use
- Stretch uterus (multiples or too much amniotic fluid)
- A breech position requiring external cephalic version
- Pronged labor
Complications
| Maternal | Fetal |
|---|---|
| Major maternal blood loss A higher risk of Coagulopathy Longer fetal exposure to hypoxia Hysterectomy | Intraventricular hemorrhage Seizures Brain ischemia Death |
Diagnosis
- Laboratory tests:
- Hemoglobin or hematocrit
- Coagulation tests (prothrombin time, activated partial thromboplastin time, fibrinogen, thromboelastogram)
- Ultrasound
- To rule out placenta praevia, placental abruption, or spontaneous abortion
- To support the diagnosis: abnormality in the uterine wall, a hematoma next to hysterotomy scar, free fluid in the peritoneum, anhydramnios or fetal parts outside the uterus
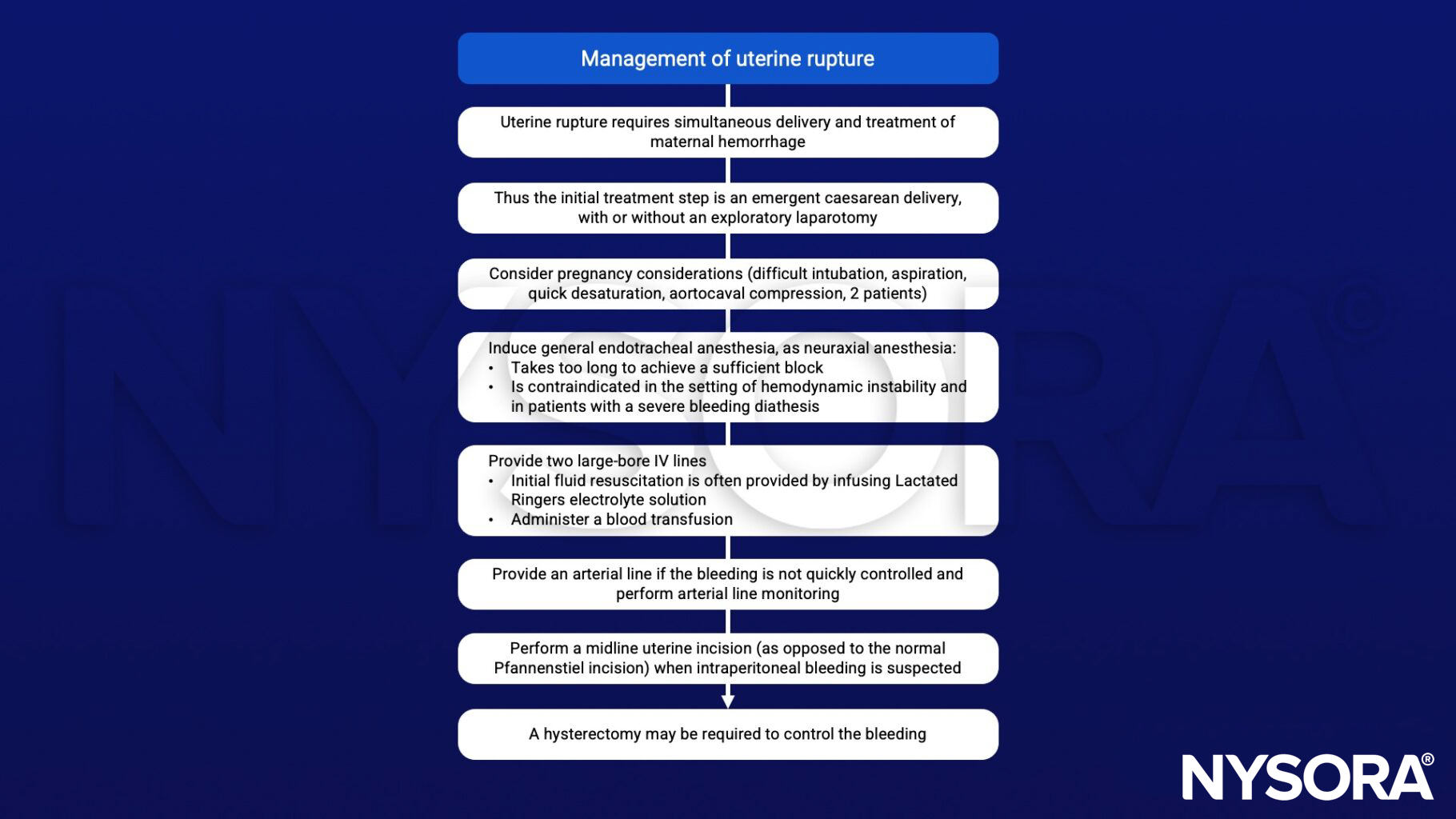
Management
Suggested reading
- Gibbins KJ, Weber T, Holmgren CM, Porter TF, Varner MW, Manuck TA. Maternal and fetal morbidity associated with uterine rupture of the unscarred uterus. Am J Obstet Gynecol. 2015;213(3):382.e1-382.e3826.
- Plaat F, Shonfeld A. 2015. Major obstetric haemorrhage. BJA Education. 15;4:190-193.
- Walfish M, Neuman A, Wlody D. 2009. Maternal haemorrhage. BJA:: British Journal of Anaesthesia. 103;1:47-56.
- Guiliano M, Closset E, Therby D, LeGoueff F, Deruelle P, Subtil D. Signs, symptoms and complications of complete and partial uterine ruptures during pregnancy and delivery. Eur J Obstet Gynecol Reprod Biol. 2014;179:130-134.












