Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About





A breakthrough randomized controlled trial by Trocheris-Fumery et al. reveals that the early administration of norepinephrine during anesthesia induction significantly reduces postoperative complications in high-risk patients undergoing major abdominal surgery.
Background
Intraoperative hypotension, a common drop in blood pressure following the induction of anesthesia, has long been associated with adverse outcomes, including:
- Myocardial injury
- Acute kidney injury (AKI)
- Increased mortality risk
Despite this, standard vasopressor regimens vary, and evidence comparing strategies for preventing such hypotension is limited.
Study overview
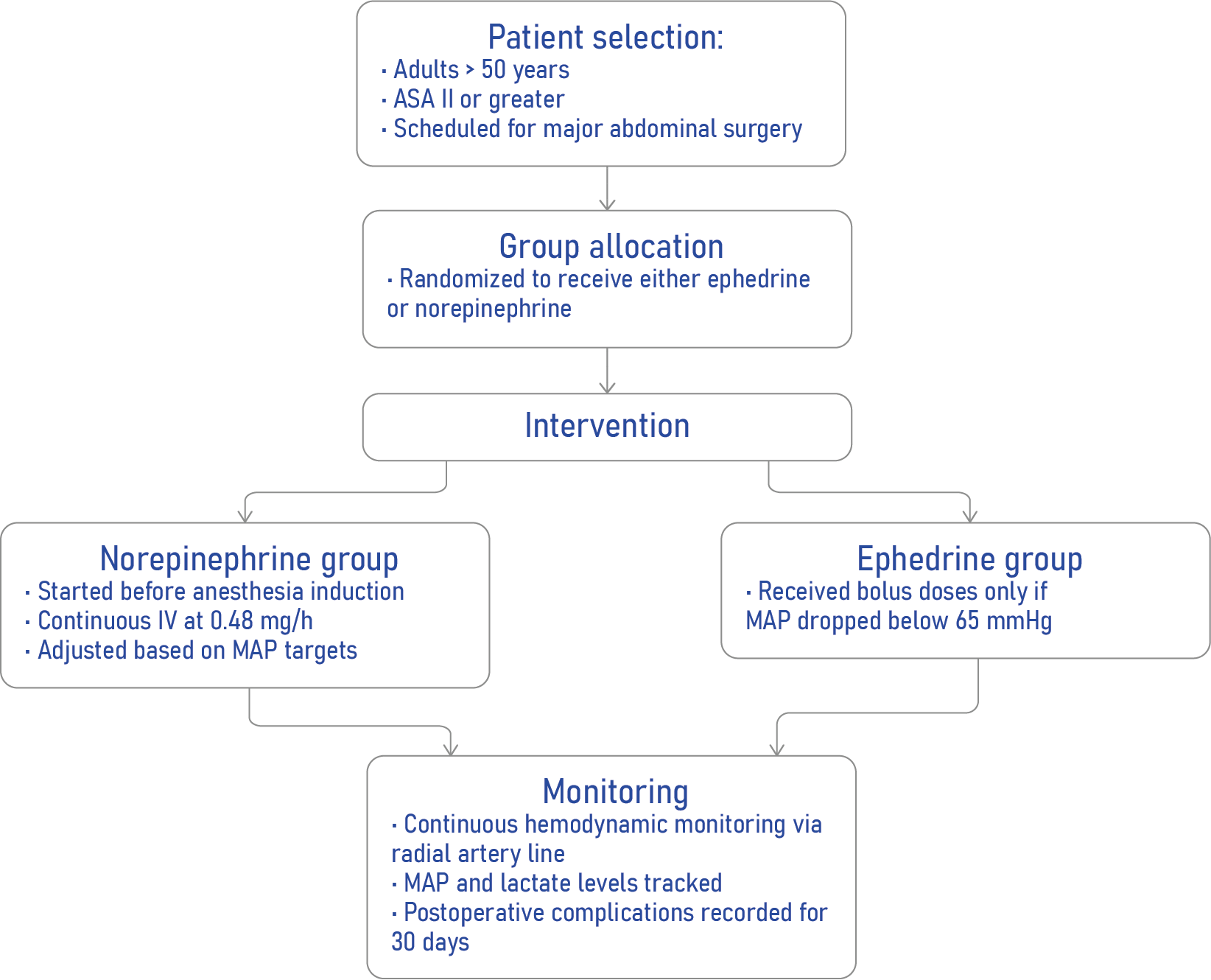
A research team at Amiens Hospital University in France conducted the EPON trial (Early Use of Norepinephrine), a single-center, randomized controlled study, to evaluate whether prophylactic norepinephrine infusion could better prevent postinduction hypotension and its associated complications compared to standard treatment with reactive ephedrine boluses.
Key study details:
- Design: Prospective, randomized, open-label, single-center
- Patients: 500 adults aged >50 undergoing major abdominal surgery
- Groups:
- Norepinephrine group: Prophylactic continuous infusion (0.48 mg/h)
- Ephedrine group: Reactive boluses (3 mg each, max 30 mg)
- Norepinephrine group: Prophylactic continuous infusion (0.48 mg/h)
How the intervention works
Core findings
Reduction in complications
- Primary endpoint: Medico-surgical complications within 30 days (Clavien–Dindo score ≥1)
- Ephedrine group: 58%
- Norepinephrine group: 44%
- Relative risk (RR): 0.58 [0.40–0.83]; P = 0.004
- Ephedrine group: 58%
Pulmonary benefits
- Postoperative pulmonary complications (PPCs) at 48 hours:
- Ephedrine: 31%
- Norepinephrine: 17%
- Ephedrine: 31%
Hemodynamic stability
- Hypotensive episodes occurred in:
- 74% of ephedrine group
- Only 15% of the norepinephrine group
- Norepinephrine also resulted in:
- Higher mean arterial pressure (MAP) post-induction
- Lower intraoperative lactate levels (suggesting better organ perfusion)
- Higher mean arterial pressure (MAP) post-induction
How norepinephrine works
Norepinephrine is a potent α1- and β1-adrenergic agonist, leading to:
- Vasoconstriction (↑ blood pressure)
- Improved cardiac output
- Stable hemodynamics during anesthesia induction
Unlike ephedrine, it avoids tachyphylaxis (diminished effect with repeated use) and is increasingly considered for first-line vasopressor use in anesthesia.
Subgroup insights
Norepinephrine was especially effective in reducing complications among:
- ASA III patients
- Men
- Patients without CKD
- Patients undergoing digestive surgery
Conclusion
Early, titrated norepinephrine infusion significantly reduces both hypotension and postoperative complications in high-risk patients undergoing major abdominal surgery. This proactive approach challenges conventional vasopressor strategies and may redefine intraoperative care in anesthesia.
Reference: Trocheris-Fumery O et al. Early Use of Norepinephrine in High-risk Patients Undergoing Major Abdominal Surgery: A Randomized Controlled Trial. Anesthesiology. 2025;143:1160-1170.
Download the AA App now to put trusted anesthesia guidance in your pocket.