Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About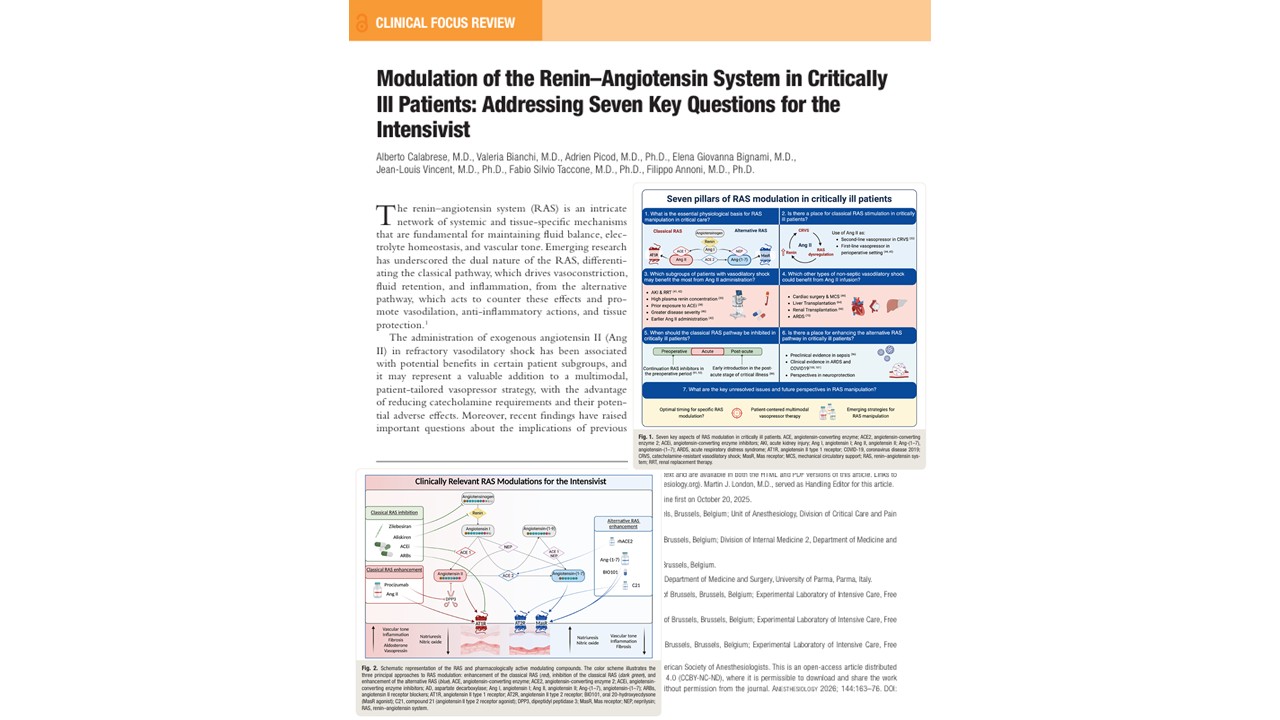





The field of intensive care medicine is undergoing a remarkable evolution with the rise of biologically targeted therapies. At the center of this transformation is the renin–angiotensin system (RAS)—a hormonal cascade historically associated with blood pressure regulation, but now recognized as a crucial therapeutic target in critically ill patients.
A recent review published Calabrese et al. 2026 in Anesthesiology provides a comprehensive synthesis of the current understanding and clinical applications of RAS modulation in ICU settings. The paper answers seven pivotal questions for intensivists, highlighting the potential of Angiotensin II (Ang II) infusion, alternative RAS activation, and tailored vasopressor strategies to revolutionize care for patients in vasodilatory shock, ARDS, and acute kidney injury (AKI).
What is the renin–angiotensin system, and why does it matter in critical illness?
The renin–angiotensin system (RAS) is a sophisticated hormonal network essential for:
- Regulating vascular tone
- Maintaining fluid and electrolyte balance
- Preserving organ perfusion in stress states
RAS comprises two main arms:
- The classical RAS pathway: Driven by ACE, Angiotensin II, and AT1 receptors, it promotes vasoconstriction, aldosterone release, fluid retention, and pro-inflammatory effects. This pathway is lifesaving during acute hypotension but harmful when persistently activated.
- The alternative (counterregulatory) RAS pathway: Mediated by ACE2, Angiotensin-(1–7), AT2R, and Mas receptors, it exerts vasodilatory, anti-inflammatory, and tissue-protective effects—this pathway balances and buffers the classical axis, especially during chronic or inflammatory diseases.
Critically ill patients often experience dysregulation of this system, particularly suppression of classical RAS during septic shock, which leads to low Ang II levels and ineffective endogenous vasopressor responses.
Angiotensin II therapy in vasodilatory shock: evidence from the ICU
The most prominent clinical use of RAS modulation is exogenous Angiotensin II administration in vasodilatory shock, especially in patients unresponsive to catecholamines.
Key evidence:
- ATHOS-3 trial: A landmark Phase 3 randomized controlled trial demonstrated that intravenous Ang II can rapidly increase mean arterial pressure (MAP) in patients with catecholamine-resistant vasodilatory shock.
- Ang II served as an effective rescue vasopressor, allowing a reduction in norepinephrine dosage, although it did not reduce 28-day mortality in the overall cohort.
These results have led to regulatory approval from the FDA and EMA, although both agencies included a black-box warning for the potential risk of thromboembolic events. Subsequent analyses, however, found no significant increase in thrombosis in patients treated with Ang II, and the event rate was very low.
Who benefits most from Ang II infusion?
Tailoring Ang II therapy requires identifying the right patient populations. Post hoc analyses from ATHOS-3 and other studies reveal specific subgroups who show greater hemodynamic and survival benefits from Ang II:
- Patients with high plasma renin concentrations
- Elevated renin indicates severe RAS suppression.
- These patients had lower 28-day mortality when treated with Ang II compared to placebo (51% vs. 70%).
- Renin may outperform lactate as a predictor of ICU mortality.
- Patients previously treated with ACE inhibitors
- ACE inhibitor users have low endogenous Ang II levels.
- Ang II administration corrects this deficiency, improving MAP.
- Renin levels dropped after Ang II infusion, indicating restored RAS feedback.
- Patients with AKI or on renal replacement therapy (RRT)
- Ang II preferentially constricts the efferent arteriole, boosting glomerular filtration rate.
- Improves survival in septic AKI requiring RRT (53% vs. 30%).
- Patients with greater disease severity
- Higher APACHE II scores and lower baseline MAP are associated with greater responsiveness.
- Earlier administration of Ang II (before high-dose norepinephrine) may yield better outcomes.
Can Angiotensin II be used beyond septic shock?
The benefits of Ang II extend into nonseptic vasodilatory states, including:
- Cardiac surgery and mechanical circulatory support (MCS)
- Cardiopulmonary bypass impairs pulmonary ACE activity, reducing Ang II production.
- Ang II helps manage vasoplegia in 5–25% of post-cardiac surgery patients.
- The ongoing PORTHOS trial is comparing Ang II with norepinephrine as a first-line vasopressor in patients with cardiac disease.
- Liver transplantation and cirrhosis
- Angiotensinogen synthesis is impaired in cirrhosis, resulting in Ang II deficiency.
- Trials are underway to assess Ang II’s role during liver transplant to combat vasodilatory hypotension.
- Ang II may reduce ischemia-reperfusion injury and stabilize perfusion.
- Some studies show reduced arrhythmias, though data on graft function remain limited.
- Acute respiratory distress syndrome (ARDS) and COVID-19
- Ang II improves oxygenation (Pao₂/FiO₂ ratio) in ARDS without altering ventilator settings.
- May optimize ventilation-perfusion matching and modulate immune response.
Inhibiting the classical RAS: when and why?
Although Ang II plays a life-saving role in shock, persistent activation of the classical RAS can be detrimental, especially in:
- Post-acute phase of AKI
- RAS overactivation leads to renal fibrosis, hypertension, and progression to chronic kidney disease (CKD).
- Reintroducing ACE inhibitors or ARBs within 6 months of AKI improves survival and renal outcomes.
- The START-or-NOT trial is evaluating the initiation of ARBs post-ICU discharge.
- COVID-19
- Continuing chronic ACEi/ARB therapy during COVID-19 is safe.
- Starting RAS inhibitors during severe COVID-19 may increase mortality.
- Perioperative settings
- ACEi/ARBs may cause intraoperative hypotension if continued before surgery.
- Three major RCTs show no significant differences in mortality or major adverse events, despite the risk of hypotension.
Unlocking the alternative RAS: a new research frontier
The alternative RAS pathway, although less explored, holds major therapeutic potential due to its:
- Anti-inflammatory
- Antifibrotic
- Vasodilatory effects
Preclinical highlights:
- Angiotensin-(1–7) reduces mortality and norepinephrine requirements in septic animals.
- Enhances renal perfusion and modulates cytokine response.
Human trials:
- Early Ang-(1–7) RCTs in COVID-19 showed no effect on the number of oxygen-free days but were underpowered.
- BIO101, a Mas receptor agonist, showed promising results: improved respiratory status and reduced mortality.
- Other agents, such as compound 21 (an AT2R agonist) and recombinant ACE2, are under evaluation.
Future directions in RAS-targeted intensive care
Despite promising data, several unresolved issues remain in implementing RAS modulation as standard ICU therapy:
- Lack of real-time RAS biomarkers
- Renin concentration is promising but not widely available.
- No point-of-care RAS profiling exists yet.
- Genetic variability and pharmacogenomics
- Certain polymorphisms in ACE and AT1R affect patient response to Ang II.
- Future strategies may involve genotype-guided therapy.
- Multimodal vasopressor strategies
- Using Ang II as a first-line vasopressor remains under investigation.
- Combining Ang II with other agents may reduce catecholamine toxicity, but it needs validation in larger trials.
- Novel therapeutic agents
- Procizumab, a monoclonal antibody targeting DPP3 (which degrades Ang II), is in early clinical trials.
- It could offer new ways to enhance endogenous Ang II levels.
Conclusion
The article by Calabrese et al. in Anesthesiology sheds light on the emerging science of RAS modulation in critical care, reinforcing the need to personalize vasopressor strategies based on a patient’s biologic and clinical profile.
As the field moves forward, we may see:
- Routine use of Ang II in select shock patients.
- Reintroduction of RAS inhibitors post-AKI to prevent CKD.
- Therapeutic use of Ang-(1–7) or Mas agonists for inflammation control.
- Development of RAS biomarker panels for ICU bedside use.
This comprehensive approach could revolutionize how we manage circulatory failure, organ dysfunction, and recovery trajectories in critically ill patients.
For more information, refer to the full article in Anesthesiology.
Calabrese A, Bianchi V, Picod A, Bignami EG, Vincent JL, Taccone FS, Annoni F. Modulation of the Renin-Angiotensin System in Critically Ill Patients: Addressing Seven Key Questions for the Intensivist. Anesthesiology. 2026 Jan 1;144(1):163-176.
Read more about the acute and chronic kidney injury in our Anesthesiology Module on NYSORA360—an essential learning resource for residents with up-to-date, practical guidance across perioperative care.