Learning objectives
- Anesthetic management of a patient with diabetes mellitus type 2
- Physiological changes due to diabetes mellitus
Definition and mechanisms
- Diabetes mellitus type 2 is a consequence of peripheral resistance to insulin action
- Is characterized by insulin resistance (hepatic, extrahepatic, or both) probably due to a decreased stimulation of glycogen synthesis in muscle by insulin, related to impaired glucose transport
- Insulin secretion and/or insulin action are thought to be deficient with excessive hepatic glucose production
- It is frequently associated with dysfunction in pancreatic β-cells responsible for insulin secretion
- The age of onset is variable, however, it is usually a disease of adults with slow onset
- Ketoacidosis is uncommon
Physiological changes
| Musculoskeletal system | Stiff joint syndrome (SJS) |
|---|---|
| Renal | Diabetic nephropathy |
| Neurological system | Increased risk of cerebrovascular accident (CVA) Nerve fibers at risk for ischemic injury Peripheral neuropathies |
| Autonomic neuropathy | Diabetic autonomic neuropathy Resting tachycardia Orthostatic hypotension Intestinal constipation Gastroparesis Bladder dysfunction Impaired neurovascular function Loss of autonomic response to Hypoglycemia |
| Cardiovascular system | Hypertension Coronary artery disease Silent myocardial ischemia Systolic and diastolic heart failure Congestive heart failure Peripheral vascular disease |
| Retinal | Diabetic retinopathy |
Management of diabetes mellitus type 2
- Diet
- Exercise
- Medications:
- Sulphonylureas (e.g. gliclazide)
- Biguanides (e.g. metformin)
- Thiazolidinediones (e.g. pioglitazone, rosiglitazone)
- Meglinitides (e.g. repaglinidine, nateglinide)
- Alpha-glucosidase inhibitors (e.g. acarbose, miglitol)
- Incretin mimetics:
- GLP-1 agonists (e.g. exanatide, liraglutide)
- DPP-4 inhibitors (e.g. sitagliptin and vildagliptin)
- SGLT2 inhibitors (e.g. canagliflozin, dapagliflozin, empagliflozin)
Anesthetic management
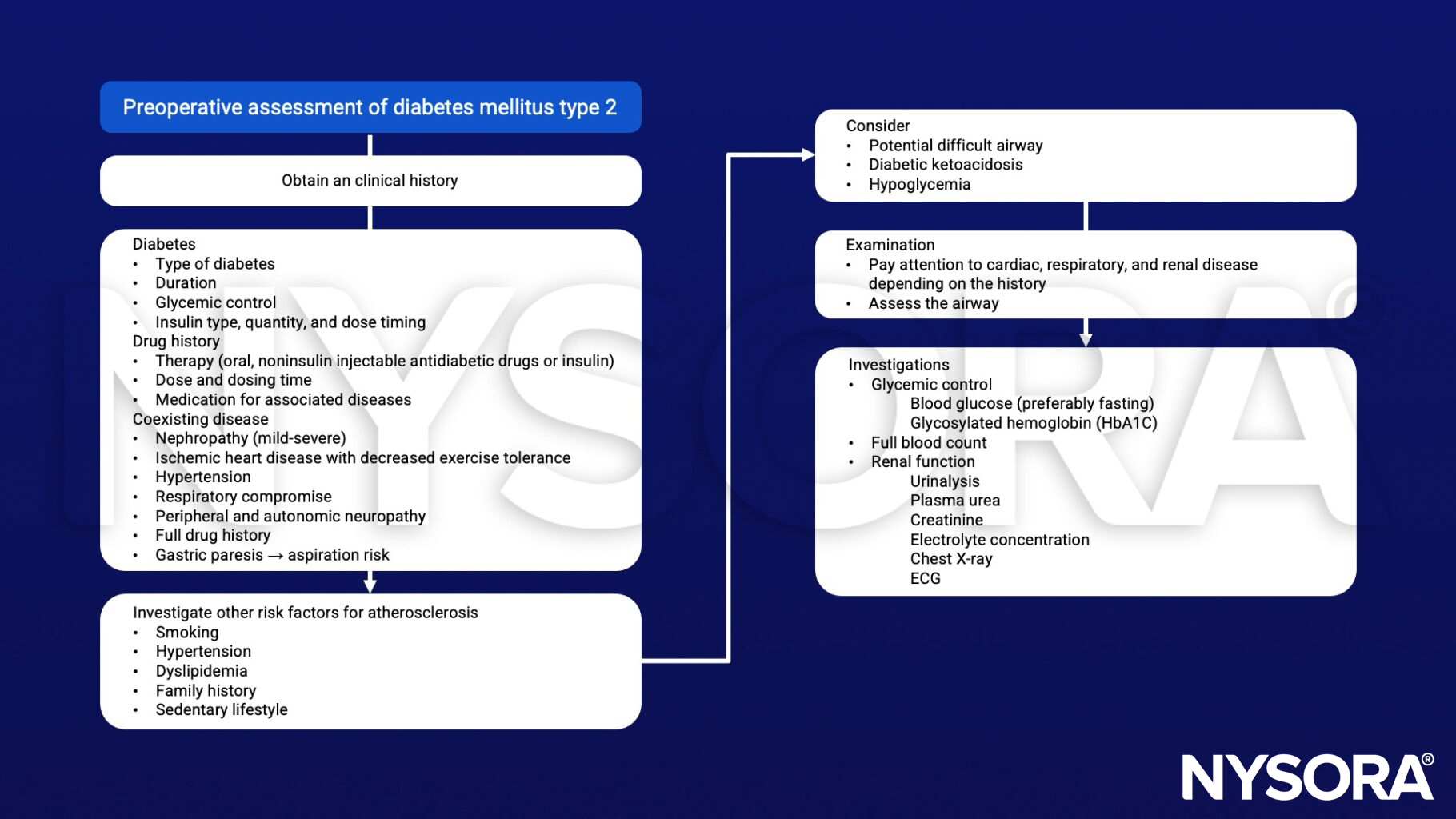
Preoperative assessment
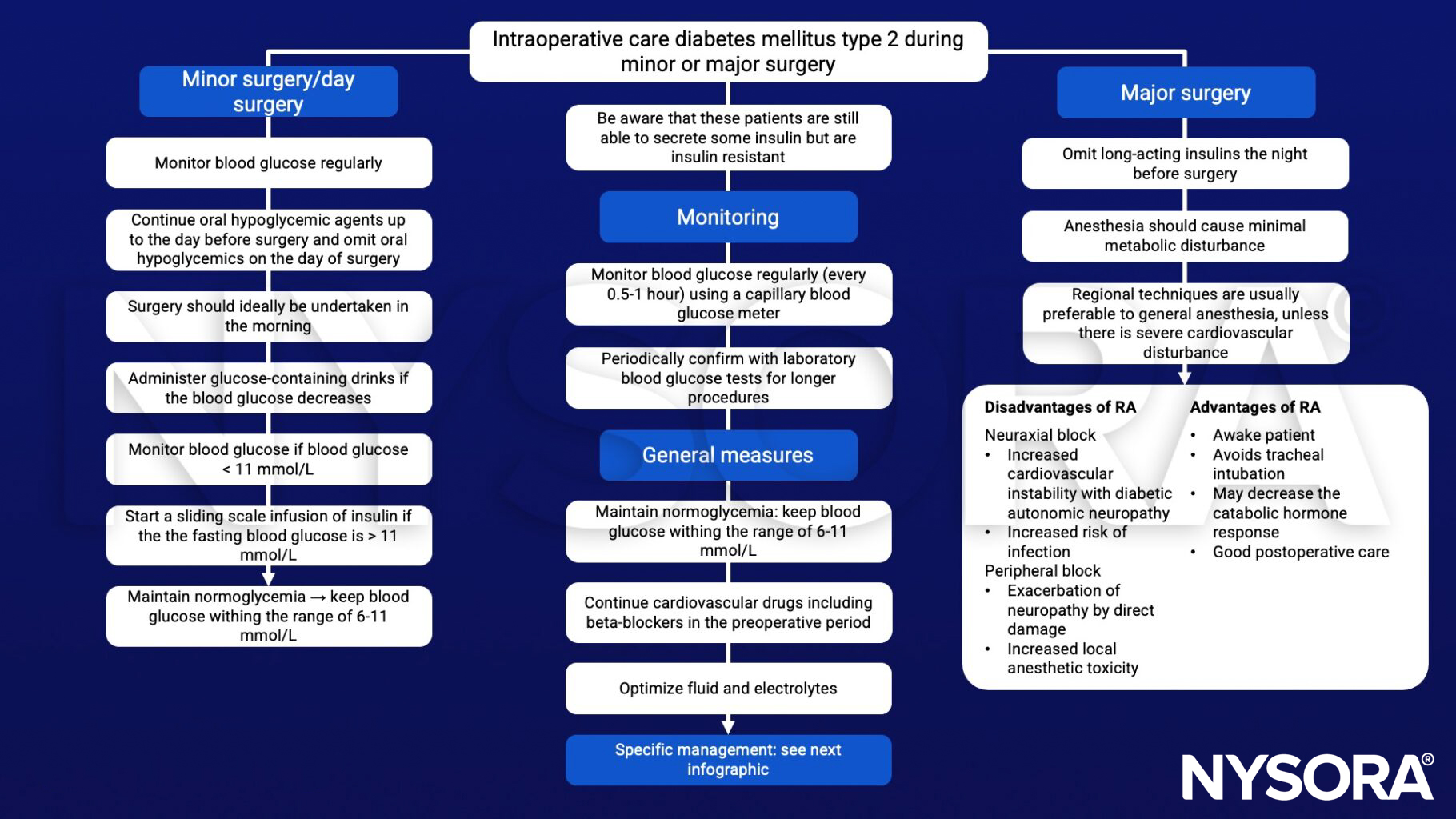
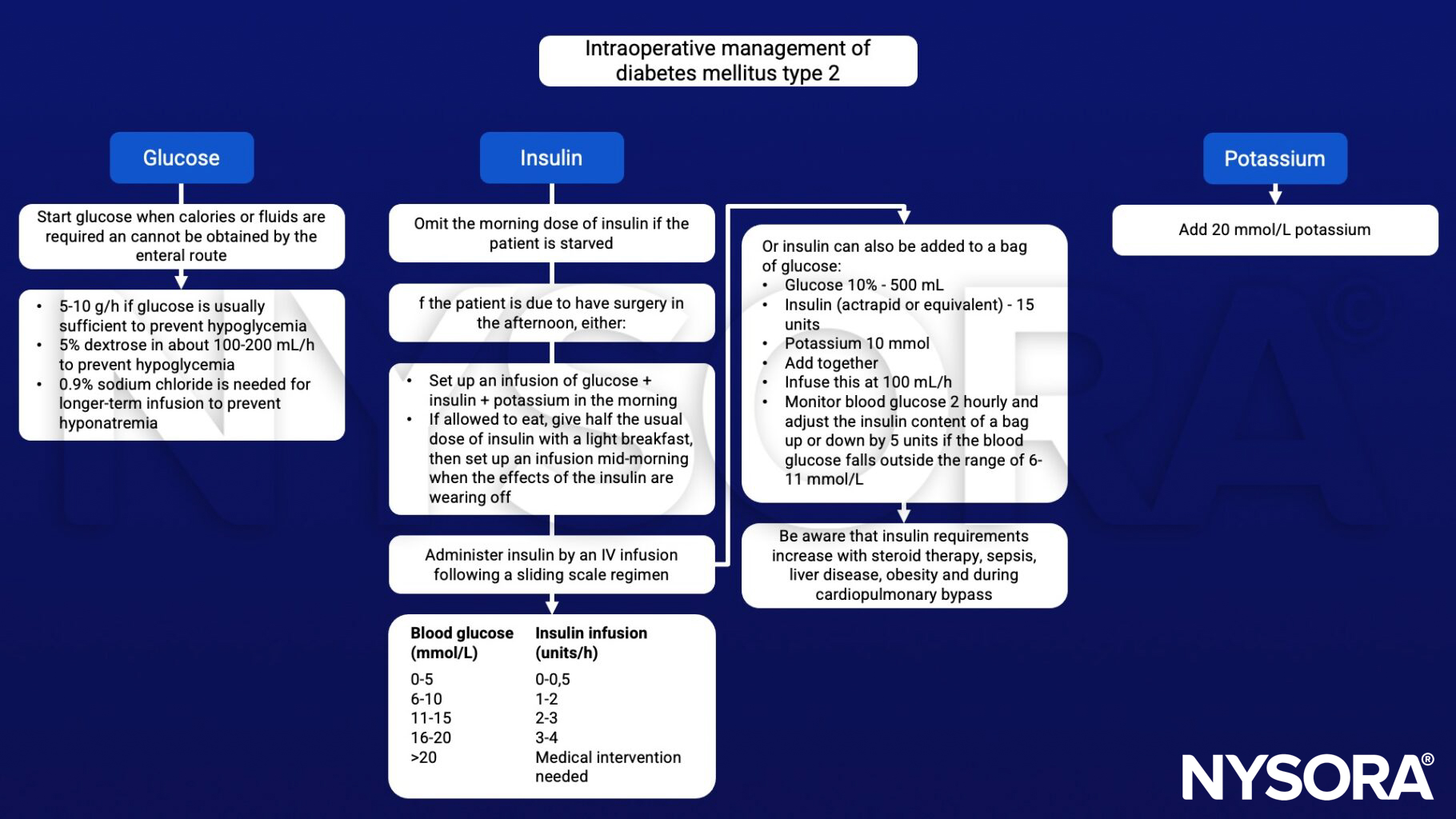
Perioperative management
Postoperative care
- Check blood glucose levels hourly until a normal diet is established
- Monitor plasma potassium 3-4 hourly, or more frequently if clinically indicated
- Administer appropriate analgesia
- Use NSAIDs with great caution as they may further impair renal function in patients with a nephropathy
- Avoid dexamethasone as it exacerbates insulin resistance
Keep in mind
HbA1c has a strong predictive value for complications of diabetes
Suggested reading
- Pollard BJ, Kitchen, G. Handbook of Clinical Anaesthesia. Fourth Edition. CRC Press. 2018. 978-1-4987-6289-2.
- Pontes JPJ, Mendes FF, Vasconcelos MM, Batista NR. Avaliação e manejo perioperatório de pacientes com diabetes melito. Um desafio para o anestesiologista [Evaluation and perioperative management of patients with diabetes mellitus. A challenge for the anesthesiologist]. Braz J Anesthesiol. 2018;68(1):75-86.
- Cornelius BW. Patients With Type 2 Diabetes: Anesthetic Management in the Ambulatory Setting: Part 2: Pharmacology and Guidelines for Perioperative Management. Anesth Prog. 2017;64(1):39-44.
- Stubbs, D.J., Levy, N., Dhatariya, K., 2017. Diabetes medication pharmacology. BJA Education 17, 198–207.
- Nicholson G, Hall GM. 2011. Diabetes and adult surgical inpatients. Continuing Education in Anaesthesia Critical CAre & Pain. 11;6:234-238.
- Robertshaw HJ, Hall GM. Diabetes mellitus: anaesthetic management [published correction appears in Anaesthesia. 2007 Jan;62(1):100]. Anaesthesia. 2006;61(12):1187-1190.
- McAnulty GR, Robertshaw HJ, Hall GM. Anaesthetic management of patients with diabetes mellitus. Br J Anaesth. 2000;85(1):80-90.
Clinical updates
Rajan et al. (A&A, 2024) update perioperative blood glucose management for adults with diabetes undergoing ambulatory surgery, recommending intraoperative glucose targets of 180–250 mg/dL tailored to surgical invasiveness and comorbidity burden. The consensus emphasizes selective continuation of metformin, withholding sulfonylureas and meglitinides on the day of surgery, cautious insulin dose reduction, and the adjunctive use of continuous glucose monitors alongside point-of-care testing—highlighting a shift toward individualized, protocol-driven glycemic control in outpatient surgical settings.
- Read more about this study HERE.
Jones et al. (A&A, 2024) report that perioperative dexamethasone does not increase surgical site infection risk in diabetic patients, despite causing transient hyperglycemia. In a meta-analysis of 2,592 diabetic patients, dexamethasone was associated with reduced postoperative nausea, pain, and overall adverse events, with benefits outweighing risks in patients with HbA1c <9%. These findings support a personalized, dose-conscious approach to dexamethasone use rather than routine avoidance in patients with diabetes.
Tinsley et al. (BJA, 2025) provide updated perioperative guidance on non-insulin diabetes medications, highlighting that drug-specific risks now play a major role in anesthetic planning for patients with type 2 diabetes. The review emphasizes withholding SGLT-2 inhibitors at least 48 hours before surgery due to the risk of euglycemic diabetic ketoacidosis, cautious perioperative use of GLP-1 receptor agonists because of delayed gastric emptying and aspiration risk, and selective continuation of agents such as DPP-4 inhibitors, reinforcing the need for individualized, medication-aware perioperative glycemic management.
- Read more about this study HERE.
Rogers et al. (Anesthesiology, 2025) emphasize that the rising prevalence of type 2 diabetes in women of reproductive age has important anesthetic implications, particularly during pregnancy, labor, and surgery, where insulin resistance is markedly amplified. The review highlights the need for tighter perioperative glucose targets, cautious use or avoidance of agents that worsen insulin resistance (e.g., dexamethasone), and heightened vigilance for atypical complications such as euglycemic diabetic ketoacidosis, especially in patients using modern antidiabetic therapies, underscoring the anesthesiologist’s central role in maintaining metabolic stability and preventing perioperative morbidity.
- Read more about this study HERE.