
 Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Signs of placental abruption
- Degrees of placental abruption
- Management of placental abruption
Definition and mechanisms
- Hemorrhage arising from the premature separation of a normally situated placenta
- Separation of the placental bed from the decidua basalis before delivery of the fetus
- Occurs in 1% of pregnancies
- Leading cause of vaginal bleeding in the latter half of pregnancy
- Emergency with high maternal and fetal morbidity/mortality
- Major complications:
- Hemorrhagic shock
- Acute kidney injury
- Coagulopathy
- Fetal demise
- Maternal death
- Delivering premature infant
- Transfusion-associated complications
- Hysterectomy
- Recurrence has been reported in 4 to 12% of cases
Signs and symptoms
- Key diagnostic factors:
- Vaginal bleeding (although about 20% of cases have no bleeding)
- Uterine tenderness
- Rapid contractions
- Abdominal pain
- Fetal heart rate abnormalities
- The clinical implications of a placental abruption vary based on the extent of the separation and the location of the separation
- Placental abruption can be complete or partial and marginal or central
- The classification of placental abruption is based on the following clinical findings:
Class 0: asymptomatic
Class 1: mild Class 2: moderate Class 3: Severe
Discovery of a blood clot on the maternal side of a delivered placenta
Diagnosis is made retrospectively No sign of vaginal bleeding or a small amount of vaginal bleeding
Slight uterine tenderness
Maternal blood pressure and heart rate within normal limits
No signs of fetal distress No sign of vaginal bleeding to a moderate amount of vaginal bleeding
Significant uterine tenderness with tetanic contractions
Change in vital signs: maternal tachycardia, orthostatic changes in blood pressure
Evidence of fetal distress
Clotting profile alteration: hypofibrinogenemia No sign of vaginal bleeding to heavy vaginal bleeding
Tetanic uterus/board-like consistency on palpation
Maternal shock
Clotting profile alteration: hypofibrinogenemia and coagulopathy
Fetal death
- Classification of 0 or 1 is usually associated with a partial, marginal separation
- Whereas, classification of 2 or 3 is associated with complete or central separation
Stages of hypovolemic shock
I Compensated II Mild III Moderate IV Severe
Blood loss <15%; 750–1000 ml 15–30%; 1000–1500 ml 30–40%; 1500–2000 ml >40%; ≥2000 ml
Heart rate (beats/min) <100 >100 >120 >140
Arterial pressure Normal; vasoconstriction redistributes blood flow, slight increase in diastolic pressure Orthostatic changes in arterial pressure, vasoconstriction intensifies in non-critical organs (skin, muscle, gut) Markedly decreased (systolic arterial pressure <90 mm Hg); vasoconstriction decreases perfusion to abdominal organs Profoundly decreased (systolic arterial pressure <80 mm Hg); decreased perfusion to vital organs (brain, heart)
Respiration Normal Mild increase Moderate tachypnea Marked tachypnea—respiratory failure
Mental status Normal, slightly anxious Mildly anxious, agitated Confused, agitated Obtunded
Urine output (ml/h) >30 20-30 <20 None (anuria)
Capillary refill Normal (<2 s) >2 s; clammy skin Usually >3 s; cool, pale skin >3 s; cold, mottled skin
Risk factors
- Health history and past obstetrical events:
- Smoking
- Cocaine use
- Maternal age over 35 years
- Hypertension
- Placental abruption in a prior pregnancy
- Current pregnancy:
- Multiple gestation pregnancies
- Polyhydramnios
- Preeclampsia
- Sudden uterine decompression
- Short umbilical cord
- Unexpected trauma
Causes
- The exact etiology is unknown
- Specific cause is often unknown
- Trauma or injury to the abdomen
- Rarely a short umbilical cord or rapid loss of amniotic fluid
Diagnosis
- Clinical signs/symptoms
- Ultrasound (however low sensitivity)
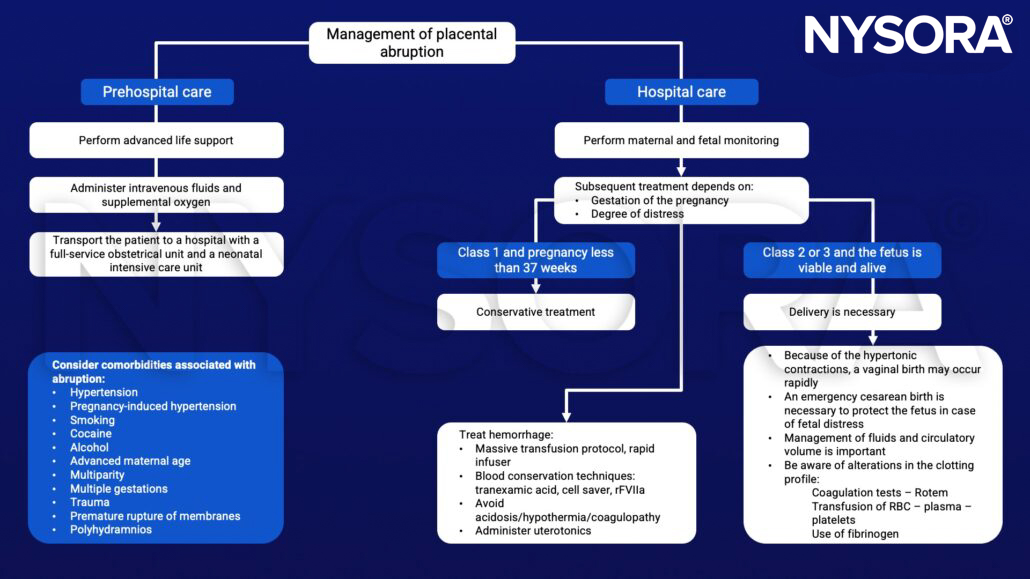
Management
Suggested reading
- Schmidt P, Skelly CL, Raines DA. Placental Abruption. In: StatPearls. Treasure Island (FL): StatPearls Publishing; April 1, 2022.
- Walfish, M., Neuman, A., Wlody, D., 2009. Maternal haemorrhage. British Journal of Anaesthesia 103, i47–i56.












