
 Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Define tetralogy of Fallot
- Describe the signs and symptoms of tetralogy of Fallot
- Understand the pathophysiology of tetralogy of Fallot
- Anesthetic management of a patient with tetralogy of Fallot
Definition and mechanisms
- Tetralogy of Fallot (TOF) is one of the most congenital heart defects (10%), resulting in a right-to-left shunt characterized by
- Large non-restrictive ventricular septal defect (VSD)
- Valvular, subvalvular, or supravalvular pulmonary stenosis, causing right ventricular outflow tract obstruction (RVOTO)
- Right ventricular hypertrophy
- Overriding aorta
- Cyanotic heart disease
- TOF often presents with low birth weight and prematurity
- TOF may present with other anatomical anomalies
- Stenosis of the left pulmonary artery (40%)
- Bicuspid pulmonary valve (60%)
- Right-sided aortic arch (25%)
- Coronary artery anomalies (10%)
- Patent foramen ovale or atrial septal defect → pentalogy of Fallot
- Atrioventricular septal defect
- Partially or totally anomalous pulmonary venous return
Signs and symptoms
- Right-to-left shunt
- Cyanosis (bluish coloration of the skin caused by hypoxemia)
- Hypoxia/low SpO2 (60-90%) with little or no response to oxygen therapy
- Shortness of breath and rapid breathing, especially during feeding or exercise
- Heart murmurs (pansystolic and ejection systolic)
- Abnormal, rounded shape of the nail bed in the fingers and toes (clubbing)
- Poor weight gain
- Tiring easily during feeding or exercise
- Irritability
- Prolonged crying
- Polycythemia
- Baby may turn blue with breastfeeding or crying
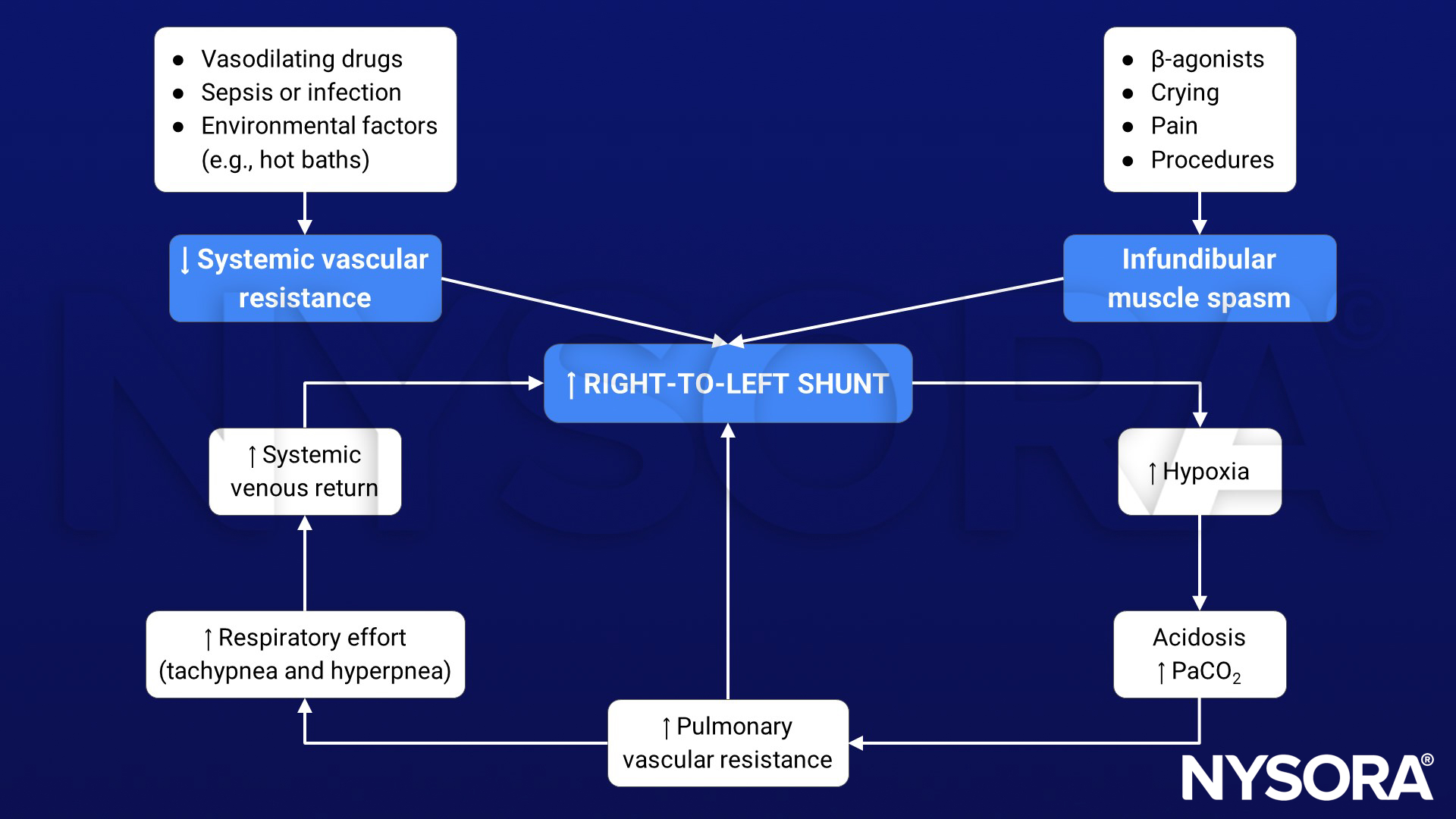
Tet spells
- Infants and children with unrepaired TOF may develop tet spells → acute hypoxia spells, characterized by shortness of breath, cyanosis, agitation, and loss of consciousness (syncope)
- Initiated by any event (i.e., crying, bowel movements, anxiety, pain, dehydration, or fever) that leads to decreased oxygen saturation or that causes decreased systemic vascular resistance (SVR) → increased shunting through the VSD (increased right-to-left shunt)
- Decrease in frequency after the first four years of life
- Older children will squat to increase the SVR → temporary reversal of shunt
Complications
- Endocarditis
- Arrhythmias (particularly supraventricular or ventricular)
- Pulmonary regurgitation
- Dizziness, fainting, or seizures due to hypoxemia
- Delayed growth and development
Risk factors
- Viral illness during pregnancy (rubella)
- Maternal alcohol consumption
- Maternal smoking
- Maternal diabetes mellitus or gestational diabetes
- Maternal age >40
- Family history of TOF
- Down syndrome or DiGeorge syndrome
- Tracheoesophageal fistula or VACTERL association
- Male gender
Pathophysiology
Anatomy of TOF allows mixing of blood between the pulmonary and systemic circulations (usually at VSD) → right-to-left shunt adding deoxygenated blood to the systemic circulation → cyanosis
Diagnosis
- Many patients are diagnosed prenatally
- Chest radiography: Abnormal “coeur-en-sabot” (boot-like) appearance of the heart
- Electrocardiogram: Right ventricular hypertrophy along (tall R-waves in lead V1 and deep S-waves in lead V5-V6) with right-axis deviation
- Echocardiogram: Presence of VSD, right ventricular hypertrophy, and aortic override; color Doppler to measure the degree of pulmonary stenosis
Treatment
- Surgical repair
- Patch closure of the VSD to separate the pulmonary and systemic circulation
- Enlargement of the RVOT (increase the size of the pulmonary valve and pulmonary arteries) to relieve RVOTO
- Usually takes place in the first year following birth, at age 3-6 months
- Intraoperative transesophageal echo to evaluate the VSD closure and RVOT
Long-term complications after TOF surgery
- Chronic pulmonary valve regurgitation
- Tricuspid valve regurgitation
- VSD that may continue to leak after repair or may need re-repair
- Hypertrophic right or left ventricle and dysfunction
- Arrhythmias
- Coronary artery disease
- Aortic root and valve dilation
- Sudden cardiac death
Management
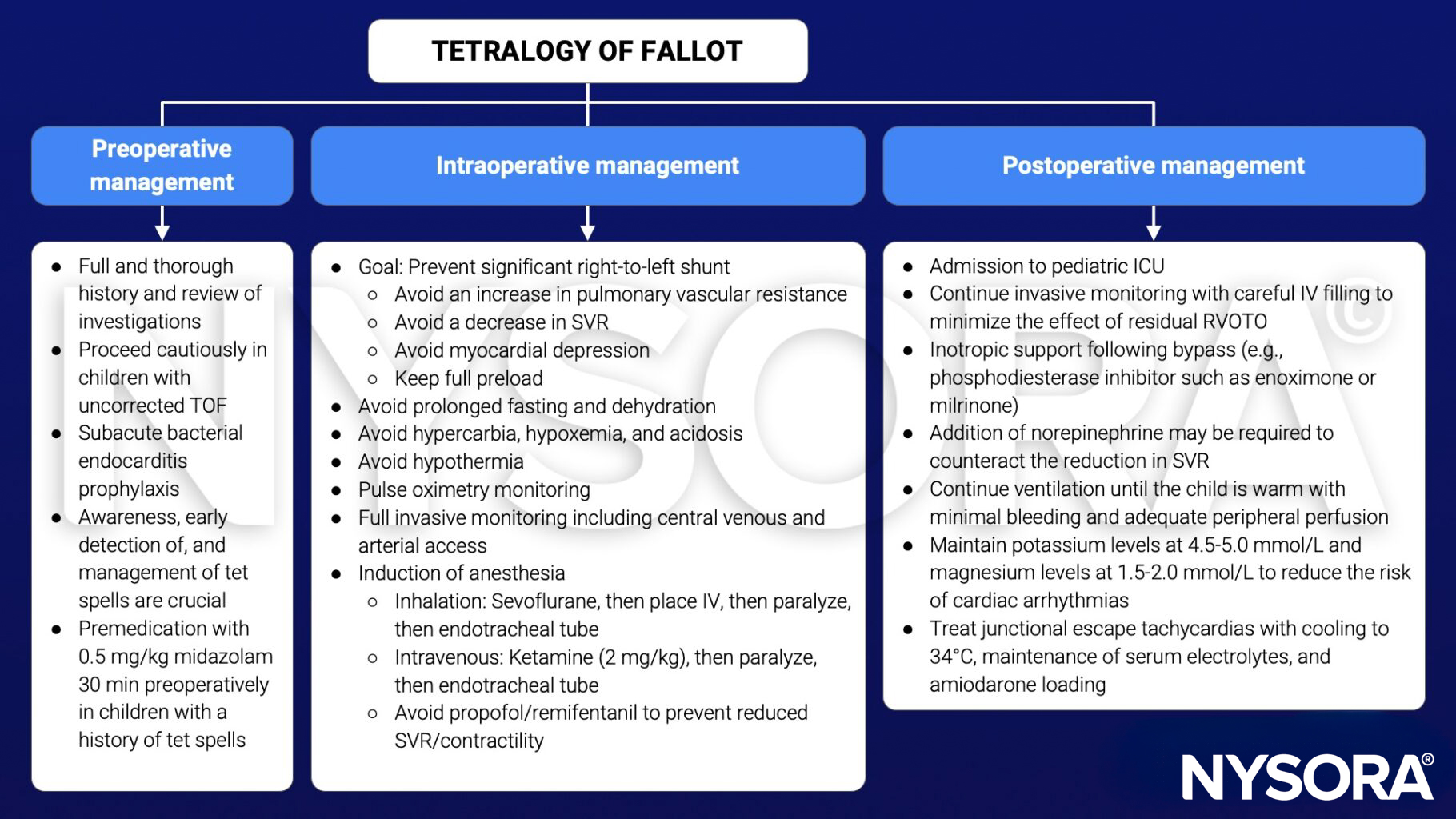
Management of tet spells during anesthesia
- Goal: Increase oxygenation, improve cardiac output, and reduce infundibular spasm and right-to-left shunt
- Give 100% oxygen and check the endotracheal tube position
- Deepen anesthesia and give an opiate bolus (e.g., 0.1 mg/kg morphine)
- Fluid bolus
- Vasopressor therapy (e.g., 5 mcg/kg phenylephrine)
- β-blockers (e.g., 0.1-0.3 mg/kg propranolol)
- Knee-to-chest flexion position
Keep in mind
- TOF is characterized by the presence of a VSD, RVOTO, right ventricular hypertrophy, and overriding aorta
- TOF is one of the most common cyanotic heart defects
- Prevention of tet spells is the key for safe anesthesia
Suggested reading
- Wilson R, Ross O, Griksaitis MJ. Tetralogy of Fallot. BJA Educ. 2019;19(11):362-369.
- Pollard BJ, Kitchen G. Handbook of Clinical Anaesthesia. 4th ed. Taylor & Francis group; 2018. Chapter 2 Cardiovascular system, Tully RP and Turner R.











