Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Define polycythemia
- Describe the classification of polycythemia
- Anesthetic management of a patient with polycythemia
Definition and mechanisms
- Polycythemia or erythrocytosis is an increase in red blood cell mass, and is associated with an increase in hemoglobin concentration (Hb) and hematocrit (Hct)
- The condition increases blood viscosity and can reduce cerebral blood flow
Classification
- Absolute polycythemia (increased red cell mass)
- Primary (polycythemia vera; PV)
- Secondary
- Idiopathic
- Apparent polycythemia (normal red cell mass)
- Reduced plasma volume
Primary polycythemia
- PV is characterized by the clonal proliferation of myeloid cells
- >95% of patients have a genetic mutation of JAK2 → stimulates overproduction of erythrocytes, platelets, and granulocytes
- JAK2 mutation is not specific for PV, also found in patients with primary thrombocytosis and primary myelofibrosis
- Clinical manifestations result from thrombotic episodes secondary to increased blood viscosity
- Production of immature platelets with variable function and acquired von Willebrand’s disease (vWD) are thought to be behind the bleeding tendency
- Associated laboratory findings
- Thrombocytosis
- Leukocytosis
- Elevated lactate dehydrogenase
- Clinical features
- Hypertension (46%)
- Splenomegaly (36%)
- Pruritus (36%)
- Erythromelalgia (29%)
- Arterial thrombosis (16%)
- Venous thrombosis (7%)
- Hemorrhage (4%)
- Facial plethora
- Hepatomegaly
- Gout
Secondary polycythemia
- Increased red cell mass is due to increased erythropoietin (EPO) production
- Compensatory mechanism in response to chronic tissue hypoxia or inappropriate production of EPO by the kidneys
- Causes include
- Chronic obstructive pulmonary disease (COPD)
- Obstructive sleep apnea (OSA)
- Cyanotic heart disease
- Altitude
- Renal artery stenosis
- Renal tumors
- Transplanted kidneys
Idiopathic polycythemia
- Increased red cell mass without an identifiable cause
- Patients are more commonly male and >50% present with vascular occlusive complications
Apparent polycythemia
- Reduced plasma volume results in an increased Hct and Hb on laboratory tests, but the red cell mass is normal
- Associated with the following clinical conditions
- Obesity
- Hypertension
- Smoking
- Excessive alcohol intake
- Diuretic use
Signs and symptoms
- Fatigue
- Headaches
- Dizziness
- Episodic blurred vision
- Red skin (particularly on the face, hands, and feet)
- Peripheral tingling, or burning and itching
- Hypertension
- Mucosal cyanosis
- Bruising
- Petechiae
- Unusual bleeding, nosebleeds
- Enlarged spleen or liver
Complications
- Pulmonary embolism
- Deep vein thrombosis
- Increased risk of heart attack and stroke
Diagnosis
| Measurement | Male | Female |
|---|---|---|
| Hemoglobin (g/L) | >185 | >165 |
| Hematocrit | >0.52 | >0.48 |
Treatment
| Classification | Treatment |
|---|---|
| Primary polycythemia | Reduce the risk of thrombosis, hemorrhage, and transformation to acute leukemia or myelofibrosis Phlebotomy or venesection (Hct <0.45) and aspirin Consider hydroxyurea or interferon alpha if the above treatments fail |
| Secondary polycythemia | Phlebotomy and management of the underlying condition (if possible) |
| Idiopathic polycythemia | Phlebotomy, cytoreductive therapy is contraindicated |
| Apparent polycythemia | Lifestyle modification and phlebotomy (if required) |
Management
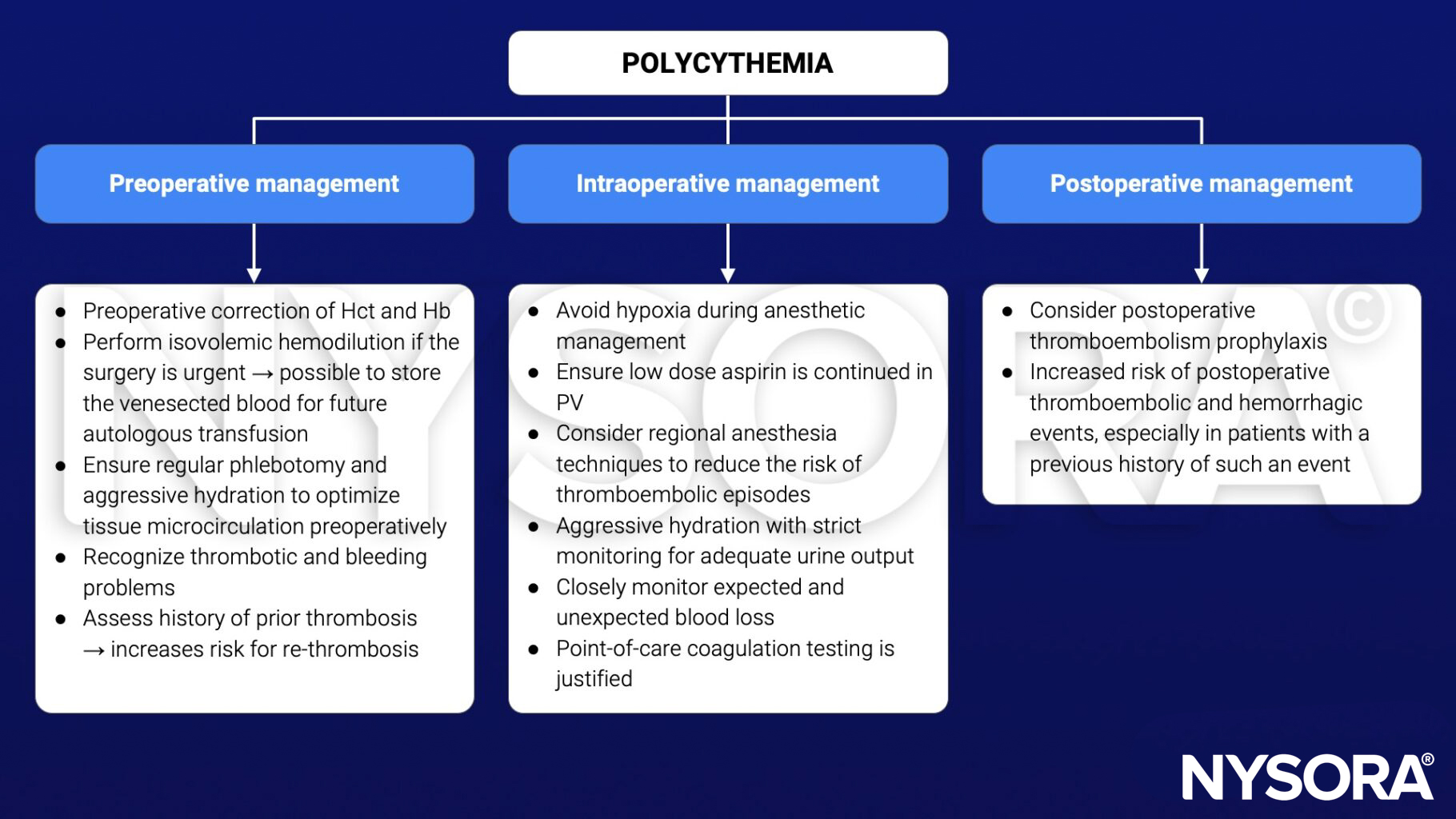
Suggested reading
- Pollard BJ, Kitchen G. Handbook of Clinical Anaesthesia. 4th ed. Taylor & Francis group; 2018. Chapter 7 The blood, Duncan A.
Clinical updates
Tremblay et al. (2025, JAMA) reaffirm that polycythemia vera (PV) is almost universally driven by JAK2 mutations (> 95%) and carries substantial risks of arterial and venous thrombosis as well as bleeding, particularly with extreme thrombocytosis and acquired von Willebrand disease. The review reinforces that all PV patients should undergo therapeutic phlebotomy targeting a hematocrit < 45% and receive low-dose aspirin, while cytoreductive therapy (hydroxyurea, interferon, or ruxolitinib) is indicated for those ≥ 60 years or with prior thrombosis.