
 Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Definition of a renal transplant
- Management of a living donor during a nephrectomy
- Management of a renal transplant recipient
Definition and mechanisms
- A renal transplant is the organ transplant of a kidney into a patient with end-stage kidney disease (ESRD)
- Classified as deceased-donor (formerly known as cadaveric) or living-donor nephrectomy (LDN)
- Improves both length and quality of life for patients with end-stage renal disease (ESRD)
- ESRD is defined as chronic kidney disease (CKD) with a glomerular filtration rate (GFR) <15 mL/min/1.73 m² or where renal replacement therapy is needed
- Diabetes is the most common cause of ESRD followed by glomerulonephritis, polycystic kidney disease, pyelonephritis, hypertension, and auto-immune disorders
- Two-year graft survival is > 80% for cadaveric and 90% for living-donor grafts and overall patient survival is > 95%
Signs and symptoms
Complications
- Bleeding
- Vascular thrombosis and stenosis
- Transplant rejection (hyperacute, acute, or chronic)
- Ureteral obstruction
- Urinary leakage
- Infections and sepsis due to immunosuppression
- Post-transplant lymphoproliferative disorder
- Electrolyte imbalance (particularly calcium and phosphate)
- Proteinuria
- Hypertension
Management of the living donor during nephrectomy
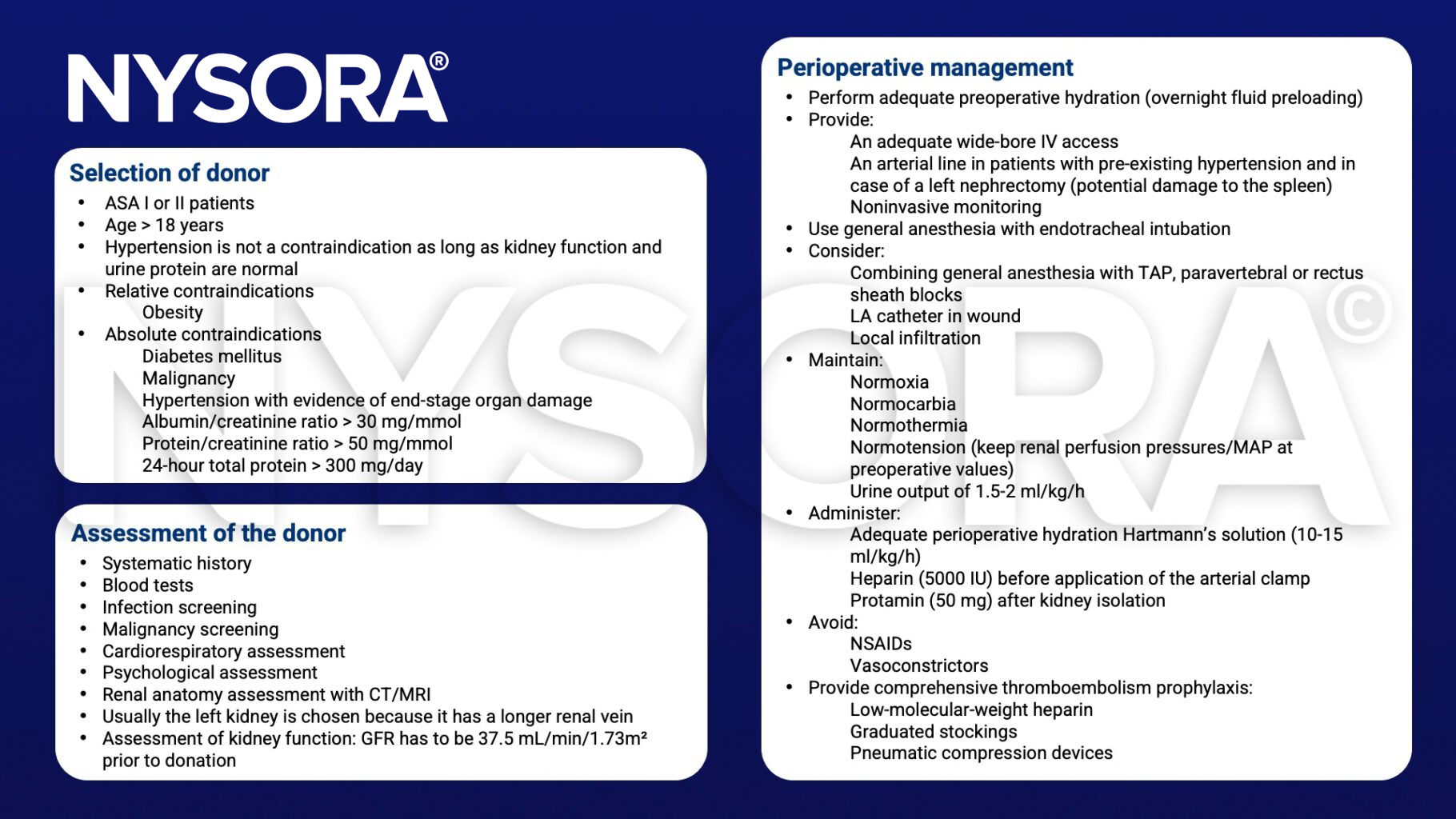
Postoperative care of the living donor
- Provide postoperative analgesia via a fentanyl PCA
- Consider a paravertebral or TAP block to complement analgesia
- Avoid NSAIDs
- Apply early mobilization along with breathing exercises and incentive spirometry
- Consider postoperative complications:
- Pulmonary embolism
- Hepatitis
- Myocardial infarction
- Arrhythmias
- Pneumonia
- Atelectasis
- Urinary tract infection
- Wound infections
- Splenic lacerations
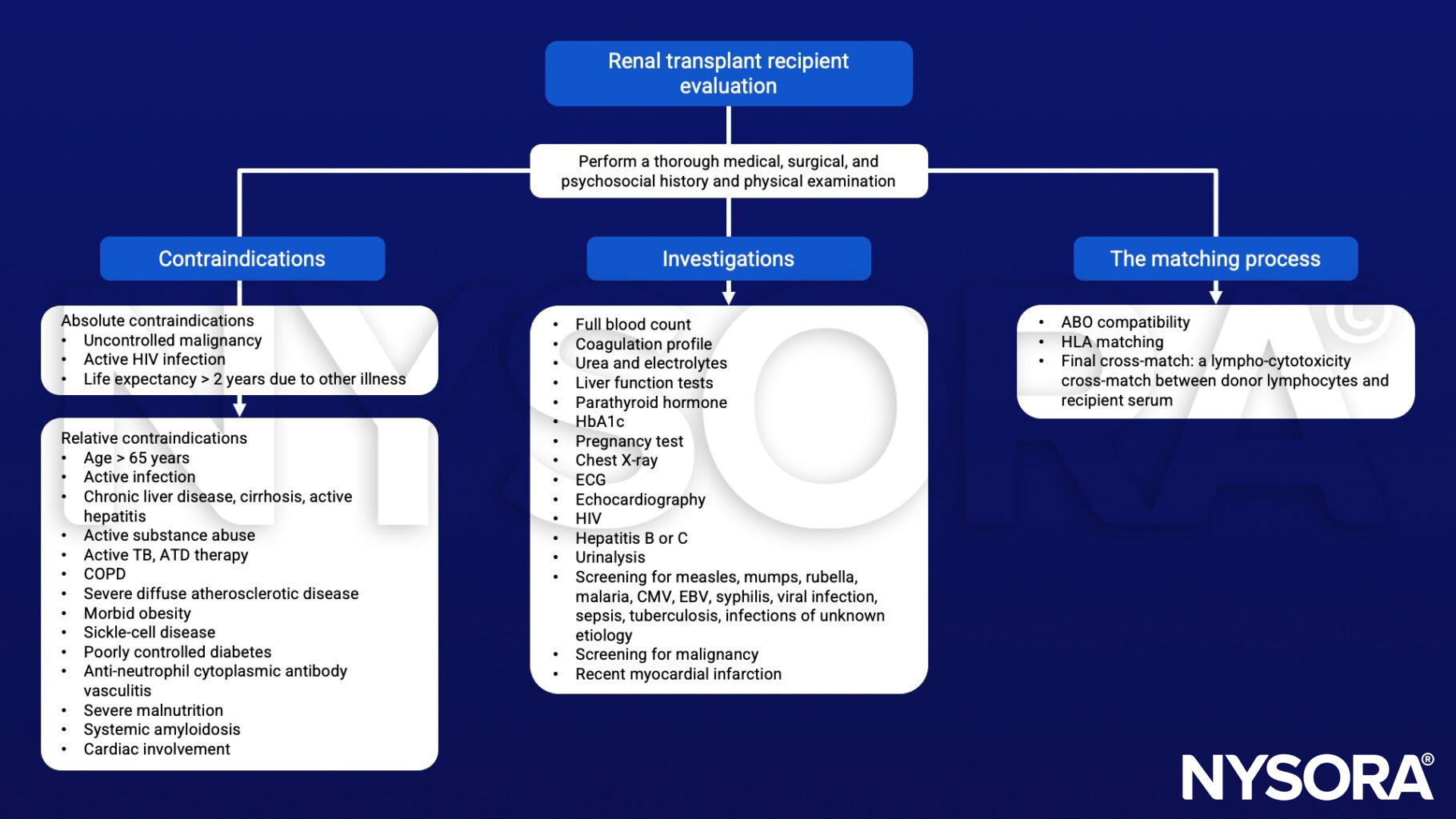
Management of the recipient


Suggested reading
- Pollard BJ, Kitchen, G. Handbook of Clinical Anaesthesia. Fourth Edition. CRC Press. 2018. 978-1-4987-6289-2.
- Mayhew D, Ridgway d, Hunter JM. 2016. Update on the intraoperative management of adult cadaveric renal transplantation. BJA education. 16;2:53-57.
- O’Brien, B., Koertzen, M., 2012. Anaesthesia for living donor renal transplant nephrectomy. Continuing Education in Anaesthesia Critical Care & Pain 12, 317–321.
- Rabey P. 2001. Anesthesia for renal transplantation. BJA CEPD Reviews. 1;1:24-17.
Clinical updates
Kim et al. (RAPM, 2024) report in a double-blinded randomized controlled trial of 88 living-donor renal transplant recipients that a unilateral anterior quadratus lumborum (QL) block did not reduce 24-hour postoperative opioid consumption or pain scores compared with a sham block when used within a multimodal analgesia regimen. Secondary outcomes were also similar between groups, suggesting routine use of the anterior QL block is not supported for analgesia after renal transplantation.
- Read more about this study HERE.
Hofer et al. (2025, A&A) report that preoperative intrathecal hydromorphone (median 100 µg) in kidney transplant recipients is associated with a 66% reduction in 72-hour postoperative opioid consumption and significantly lower pain scores at 24 and 72 hours, without increasing respiratory depression, naloxone use, or length of stay. The main trade-off was a higher incidence of postoperative nausea and vomiting, underscoring the need for proactive antiemetic prophylaxis. These findings support intrathecal opioids as a safe, opioid-sparing adjunct within evolving ERAS-style pathways for renal transplantation.
- Read more about this study HERE.











