Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Recognize common causes of TR
- Describe the signs and symptoms of TR
- Grade the severity of TR cases
- Anesthetic management of TR
Definition & mechanisms
- Tricuspid regurgitation (TR) occurs when the tricuspid valve does not close properly, causing a reversal of blood flow through the valve
- TR can be of primary or secondary origin:
- Primary (organic) TR: Pathology of the tricuspid valve complex, may be of rheumatic, degenerative, congenital, infectious, traumatic, or iatrogenic origin
- Secondary (functional) TR: Related to right ventricular dilatation and/or dysfunction, annular dilatation, and leaflet tethering, usually secondary to left-sided valvular heart disease, atrial fibrillation or pulmonary hypertension
Signs & symptoms
- Often clinically silent and symptoms usually relate to concomitant left-sided valvular heart disease
- General fatigue and reduced exercise capacity
- Upper abdominal pain
- Peripheral lower limb edema
- Systolic jugular distension
- Pulsatile hepatomegaly
- Ascites, liver failure, and cachexia may be observed in end-stage disease
- Electrocardiogram frequently shows right bundle branch block and atrial fibrillation reflects disease evolution.
Severity assessment
| Parameters | Mild | Moderate | Severe | |
|---|---|---|---|---|
| Qualitative | TV morphology | Normal/abnormal | Normal/abnormal | Abnormal/flail/large coaptation defect |
| Color flow TR jet | Small, central | Intermediate | Very large central jet or eccentric wall impinging jet | |
| CW signal of TR jet | Faint/parabolic | Dense/parabolic | Dense/triangular with early peaking (peak <2 m/s in massive TR) | |
| Semi-quantitative | VC width (mm) | Not defined | <7 | >7 |
| PISA radius (mm) | ≤5 | 6–9 | >9 | |
| Hepatic vein flow | Systolic dominance | Systolic blunting | Systolic flow reversal | |
| Tricuspid inflow | Normal | Normal | E-wave dominant (≥1 m/s) | |
| Quantitative | EROA (mm2) | Not defined | Not defined | ≥40 |
| R Vol (ml) | Not defined | Not defined | ≥45 |
Management
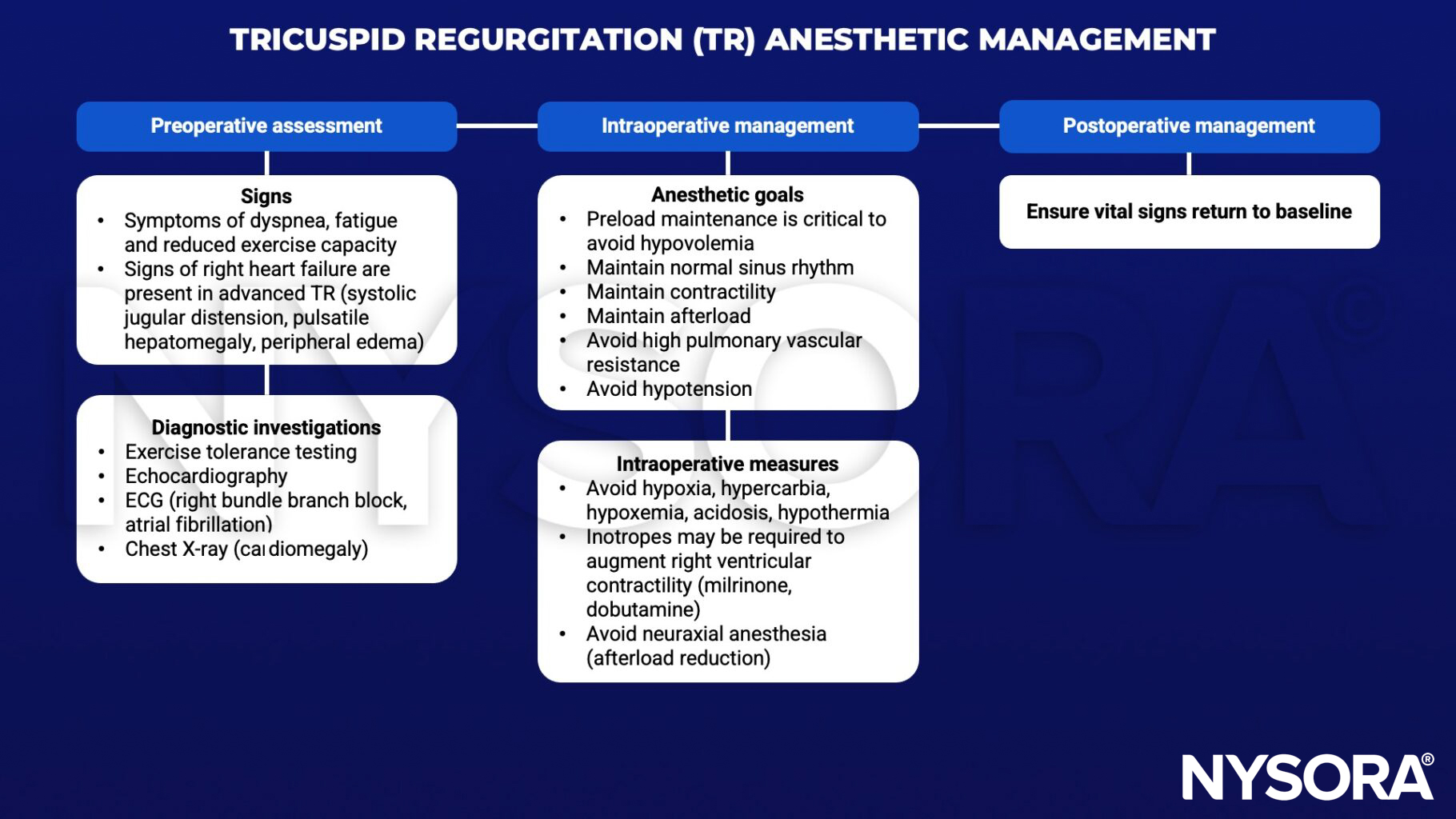
Keep in mind
Tricuspid regurgitation is most commonly secondary to other morbidities, which might require further attention.
Suggested reading
- Antunes MJ, Rodríguez-Palomares J, Prendergast B, De Bonis M, Rosenhek R, Al-Attar N, et al. Management of tricuspid valve regurgitation: Position statement of the European Society of Cardiology Working Groups of Cardiovascular Surgery and Valvular Heart Disease. European Journal of Cardio-Thoracic Surgery. 2017;52(6):1022-30.