Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Define DiGeorge syndrome
- Describe the signs, symptoms, and complications associated with DiGeorge syndrome
- Anesthetic management of a patient with DiGeorge syndrome
Definition and mechanisms
- DiGeorge syndrome, or 22q11.2 deletion syndrome, is a syndrome caused by a heterozygous microdeletion on the long arm of chromosome 22
- This deletion results in the poor development of several body systems
- 90% of cases occur due to a new mutation during early development, while 10% are inherited (autosomal dominant)
- Memory aid: CATCH-22
- Cyanotic congenital heart defect
- Abnormal facies
- Thymic aplasia or hypoplasia
- Cognitive impairment, cleft palate
- Hypoparathyroidism, hypocalcemia
- 22q11.2 deletion
Signs, symptoms, and complications
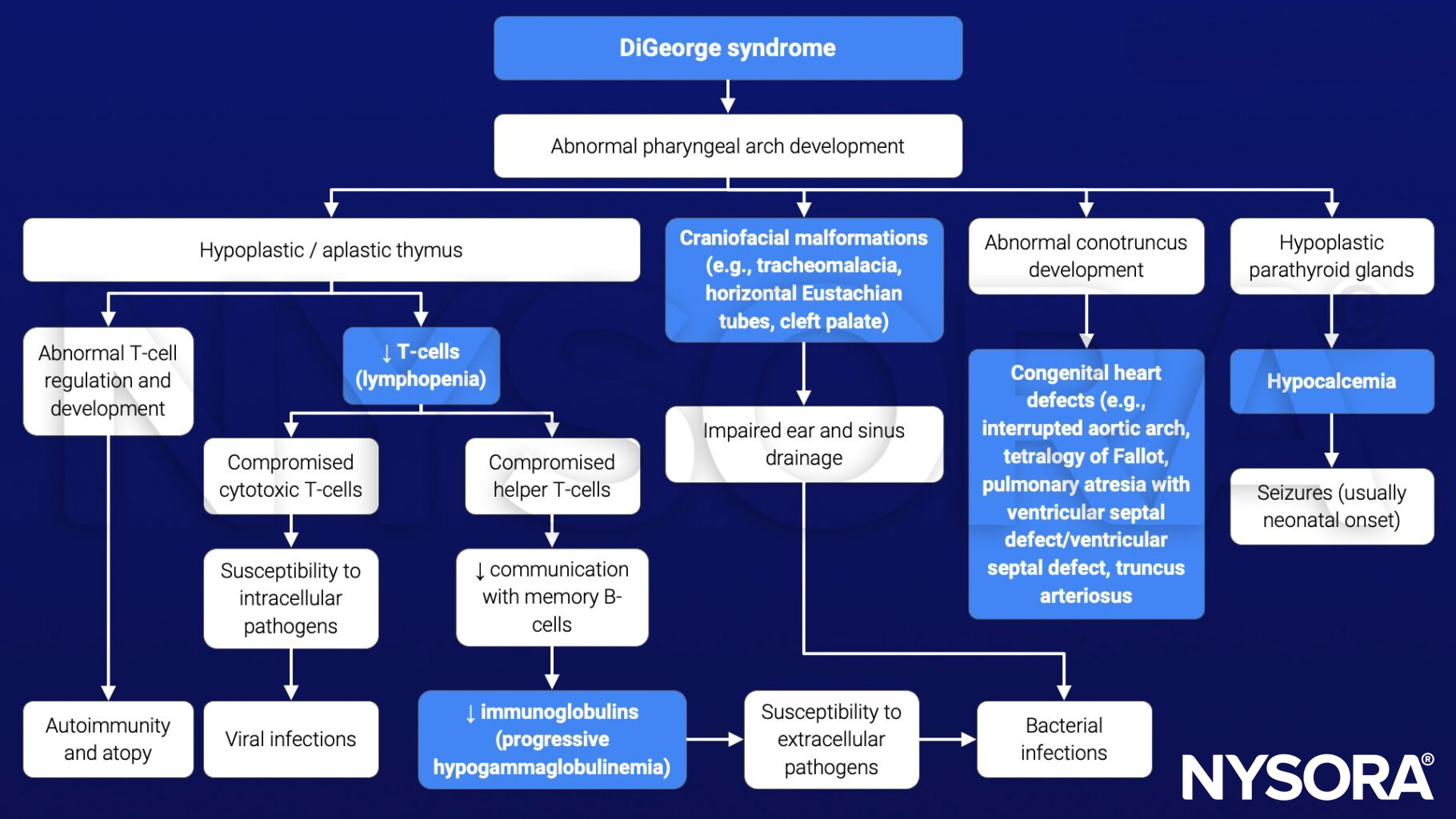
- Congenital heart disease (40%): Particularly conotruncal malformations (e.g., interrupted aortic arch, persistent truncus arteriosus, tetralogy of Fallot, and ventricular septal defect)
- Cyanosis
- Palatal abnormalities (50%): Velopharyngeal incompetence, submucosal cleft palate, and cleft palate with or without cleft lip
- Characteristic facial features (including hypertelorism): Underdeveloped chin (micrognathia and retrognathia), low-set ears, wide-set eyes, or a narrow groove in the upper lip
- Frequent infections due to thymic aplasia or hypoplasia
- Developmental delay
- Learning difficulties (90%) including cognitive deficits, attention deficit disorders
- Hypocalcemia (50%) due to hypoparathyroidism
- Significant feeding problems (30%), gastroesophageal reflux disease (GERD), and failure to thrive
- Renal anomalies (37%)
- Hearing loss
- Laryngotracheoesophageal anomalies
- Growth hormone deficiency
- Autoimmune disorders (e.g., rheumatoid arthritis or Graves disease)
- Immune disorders due to reduced T-cell numbers
- Seizures (with or without hypocalcemia)
- Skeletal abnormalities (e.g., scoliosis)
- Psychiatric disorders and behavioral problems (e.g., schizophrenia develops in 25-30% by adulthood, ADHD, autism spectrum disorder)
Pathophysiology
Treatment
There is no cure for DiGeorge syndrome, but certain individual features are treatable using standard treatments
- Hypoparathyroidism: Calcium and vitamin D supplements
- Congenital heart defects: Surgical repair soon after birth to repair the defect and improve the supply of oxygen-rich blood
- Limited thymus gland function: Infections (e.g., colds and ear infections) are generally treated as they would be in any child; normal schedule of vaccines
- Severe thymus gland function: Transplant of thymus tissue, specialized bone marrow, or specialized disease-fighting blood cells
- Cleft palate: Surgical repair
- Overall development: Speech therapy, occupational therapy, and developmental therapy
Anesthesia considerations
- Airway
- Difficult airway
- Small mouth opening, retrognathia, micrognathia
- Cleft palate, velopharyngeal insufficiency: Avoid nasal intubation
- Aspiration risk
- Pharyngeal insufficiency, GERD
- Difficult airway
- Breathing
- Nasal obstruction
- Obstructive sleep apnea (OSA)
- Circulation
- Conotruncal anomalies
- Long QT from hypocalcemia
- Disability
- Developmental delay, behavioral issues
- Tetany and seizures from hypocalcemia
- Genitourinary
- Hypocalcemia from hypoparathyroidism (especially in newborns)
- Renal anomalies
- Immunodeficiency
- Thymic hypoplasia: Recurrent infections; aseptic technique needed
- Thymic aplasia: Severe combined immunodeficiency (SCID)
- Musculoskeletal
Management
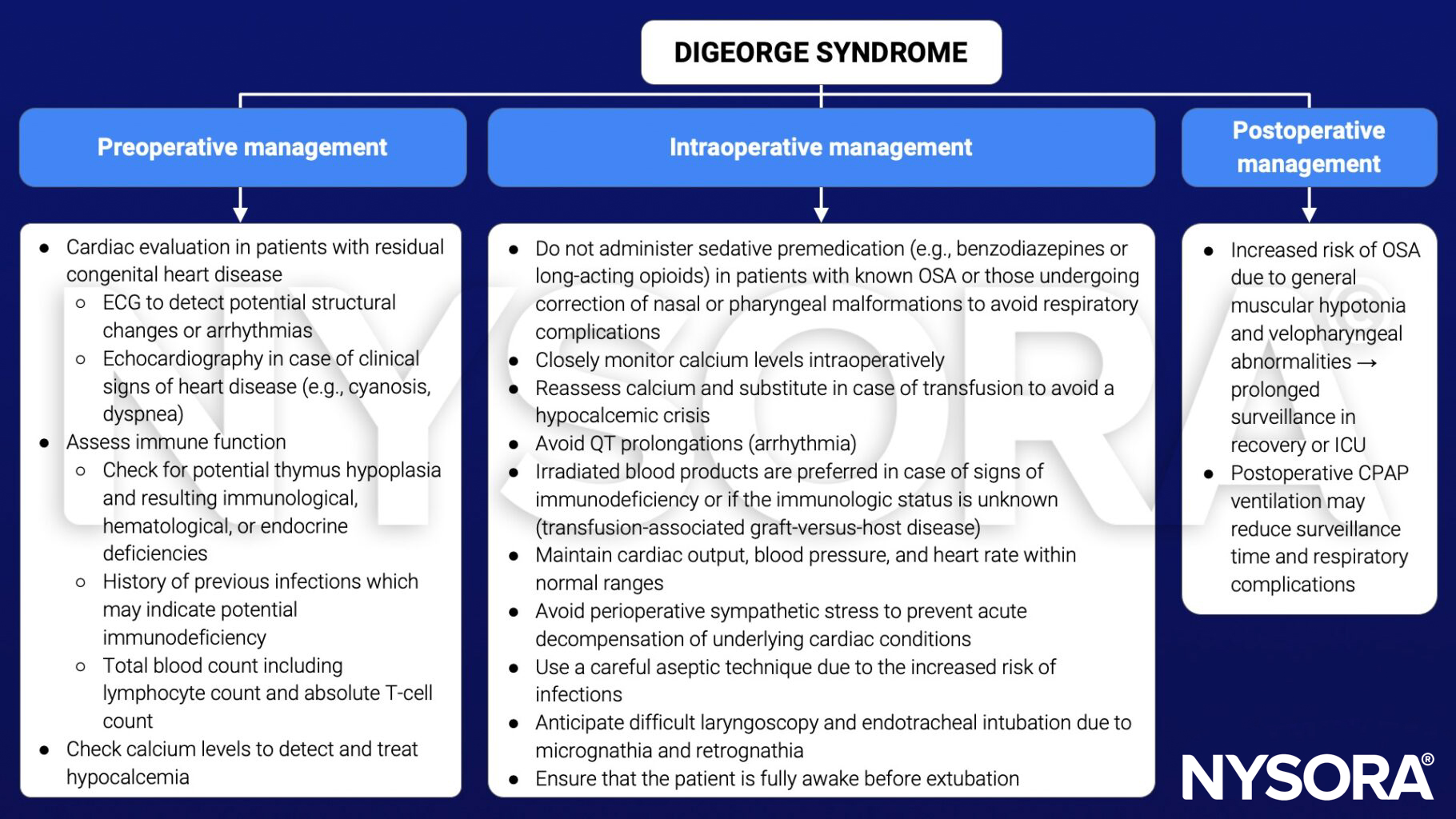
Keep in mind
- Perform a recent cardiac evaluation in patients with residual congenital heart disease
- Anticipate a difficult intubation
- Use a careful aseptic technique
- Check calcium levels
Suggested reading
- Haché M. DIGEORGE SYNDROME. In: Houck PJ, Haché M, Sun LS. eds. Handbook of Pediatric Anesthesia. McGraw Hill; 2015. Accessed March 06, 2023. https://accessanesthesiology.mhmedical.com/content.aspx?bookid=1189§ionid=70364073