Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About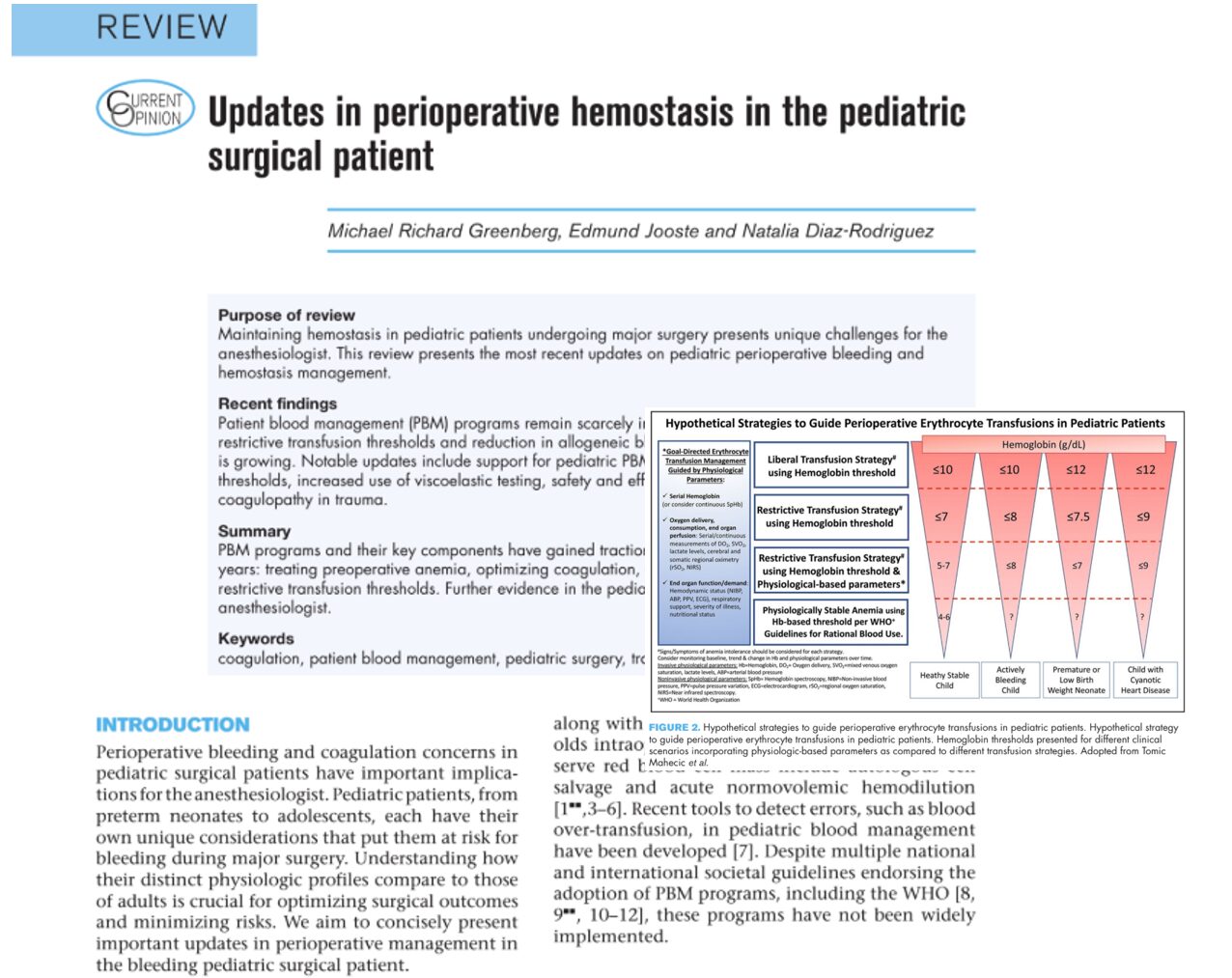





Bleeding during major pediatric surgery poses unique and complex challenges for anesthesiologists and surgical teams. From neonates to adolescents, the physiological intricacies of the pediatric hemostatic system demand tailored approaches that differ significantly from adult practices. This news post reviews recent advances in perioperative hemostasis and patient blood management (PBM) in pediatric surgical patients, offering updated guidelines and strategies for clinicians.
Understanding developmental hemostasis
Developmental hemostasis is the cornerstone for understanding pediatric bleeding risks.
- Pediatric patients have lower levels of coagulation proteins at birth.
- Despite reduced clotting factors, neonates usually maintain a balanced hemostatic system.
- Hemostatic function matures gradually, with adult-like levels achieved by 6 months of age.
- Platelet counts may be normal or elevated, but platelet function (adhesion and aggregation) is often impaired in neonates.
Clinical implication: Standard coagulation tests (aPTT, PT) may be prolonged in newborns but are not necessarily indicative of bleeding risk.
What is patient blood management (PBM)?
PBM is an evidence-based, multidisciplinary approach aimed at optimizing the care of patients who might need transfusions.
Three key pillars of PBM:
- Preoperative optimization of red cell mass (e.g., treating anemia).
- Minimization of blood loss and enhanced coagulation strategies.
- Maximizing tolerance of anemia using restrictive transfusion thresholds and physiologic support.
Despite international support (e.g., WHO guidelines), PBM adoption in pediatrics is still limited.
Preoperative considerations
- Anemia screening is vital due to its link with increased perioperative mortality.
- No universal guidelines for preoperative coagulation screening exist.
- A hematology consult is recommended if there’s a personal or family history suggestive of bleeding disorders.
Intraoperative bleeding: strategies and updates
Red blood cell transfusion
- Avoid a single transfusion trigger due to varied physiology across age groups.
- Suggested hemoglobin thresholds:
- 8 g/dl during significant intraoperative blood loss.
- 7 g/dl for stable, critically ill children.
- 8 g/dl during significant intraoperative blood loss.
- Physiologic markers (e.g., near-infrared spectroscopy) may guide decisions better than fixed thresholds.
Hemostatic blood products
1. Cryoprecipitate and fibrinogen concentrate
- Fibrinogen is the first factor to drop during major bleeding.
- Treat when fibrinogen <150 mg/dl.
- Dosing: 5–10 ml/kg of cryoprecipitate.
- Fibrinogen concentrate is an alternative, especially in cardiac surgery.
2. Fresh frozen plasma (FFP)
- Indicated in:
- Liver disease
- Vitamin K deficiency
- DIC
- Dilutional coagulopathy
- Liver disease
- A 10 ml/kg dose increases coagulation factor levels by 20%.
3. Platelets
- Use during major bleeding, severe thrombocytopenia, or platelet dysfunction.
- Transfusion dose: 10 ml/kg increases platelet count by ~150×10⁹/L.
4. Recombinant factor concentrates
- 4-factor PCC (contains factors II, VII, IX, X) is used off-label in pediatric surgery.
- Limited pediatric data, mostly from cardiac surgery.
- Thrombosis risk remains a concern.
Viscoelastic testing (VET)
- Includes technologies like ROTEM and TEG.
- Provides dynamic real-time insight into clot formation and stability.
- Faster and more comprehensive than standard lab tests.
- Age-specific reference ranges are lacking, but VET is promising in pediatric surgery.
Antifibrinolytic therapy
- Tranexamic acid (TXA) is widely used to reduce surgical blood loss.
- Dosing: 10–30 mg/kg loading dose; 5–10 mg/kg/h infusion.
- Safe in most children, including those with seizure disorders at therapeutic doses.
- Dosing: 10–30 mg/kg loading dose; 5–10 mg/kg/h infusion.
- Shown to reduce transfusions in:
- Cardiac surgery
- Spinal fusion
- Craniosynostosis procedures
- Cardiac surgery
Trauma and massive hemorrhage
Key points:
- Massive transfusion, defined as ≥40 ml/kg blood product in 24 hours, is linked to higher mortality.
- Trauma-induced coagulopathy (TIC) is now recognized as more prevalent across pediatric age groups.
- Early blood product resuscitation is prioritized over crystalloids.
- Suggested transfusion ratios: 1:1:1 or 2:1:1 for PRBCs:FFP: platelets.
Whole blood resuscitation
- Low-titer group O whole blood (LTOB) is gaining traction in pediatric trauma.
- Benefits:
- Faster delivery
- Reduced exposure to multiple products
- Potentially improved survival in massive hemorrhage
- Faster delivery
Step-by-step: managing perioperative bleeding in pediatrics
-
Preoperative
- Screen for anemia and bleeding history.
- Optimize red cell mass and coagulation.
- Screen for anemia and bleeding history.
-
Intraoperative
- Monitor blood loss.
- Use VET and lab tests for real-time decision-making.
- Apply PBM principles for transfusion thresholds.
- Monitor blood loss.
-
Postoperative
- Continue monitoring for bleeding.
- Reassess hemoglobin and coagulation status.
- Minimize unnecessary transfusions.
- Continue monitoring for bleeding.
Conclusion
Modern management of perioperative bleeding in pediatric patients emphasizes a tailored, physiology-based approach over rigid transfusion thresholds. The integration of VET, antifibrinolytics like TXA, and whole blood transfusion protocols holds promise for improving outcomes. Wider implementation of PBM programs, alongside pediatric-specific research, is crucial to standardizing care and reducing complications.
Reference: Greenberg MR et al. Updates in perioperative hemostasis in the pediatric surgical patient. Curr Opin Anaesthesiol. 2025;38:222-229.
Read more about this topic in the Anesthesia Updates section of the Anesthesia Assistant App. Prefer a physical copy? Get the latest literature and guidelines in book format. For an interactive digital experience, check out the Anesthesia Updates Module on NYSORA360!