Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About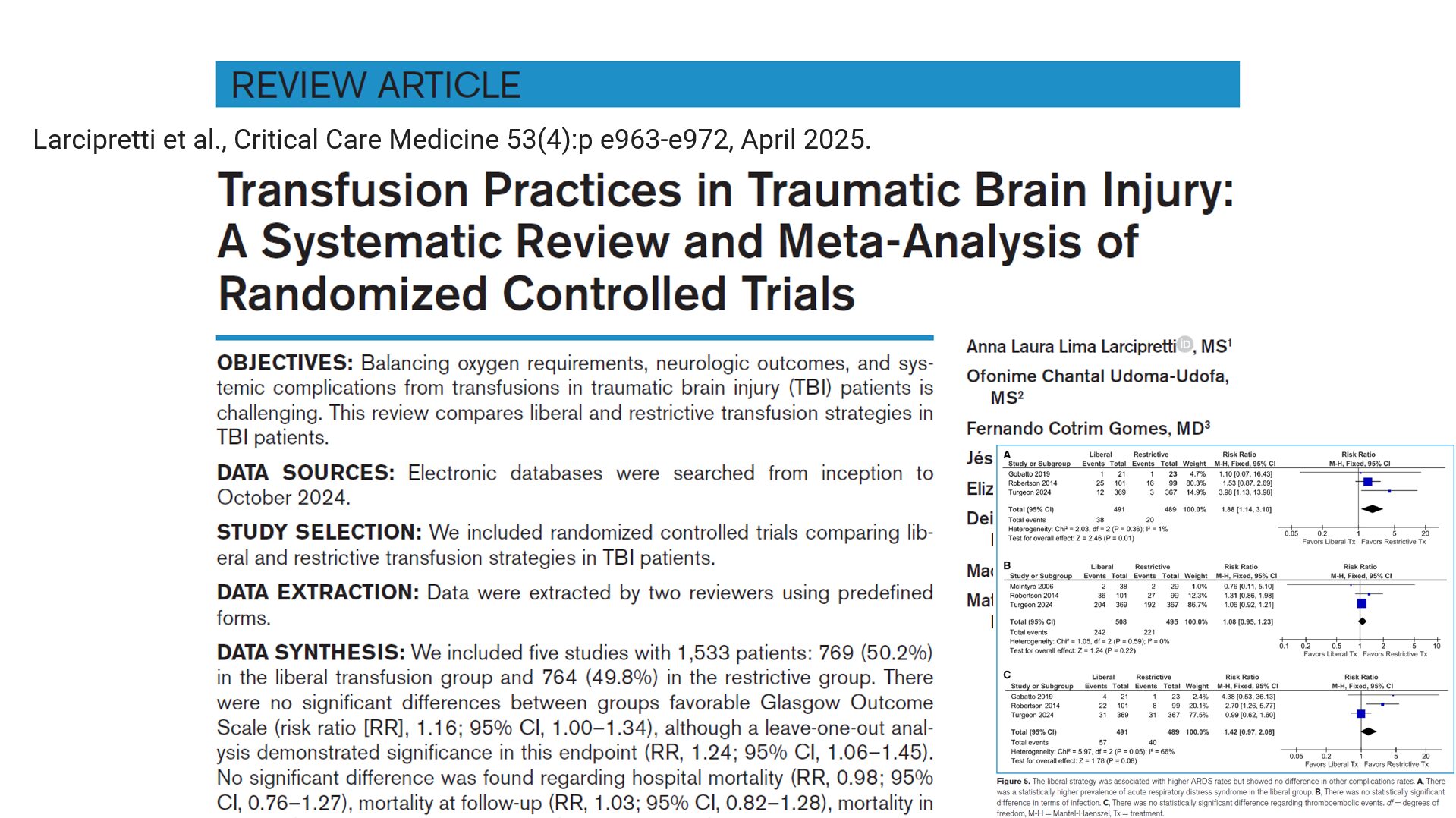

Traumatic brain injury (TBI) remains a significant global health challenge. For patients recovering in critical care settings, managing anemia through red blood cell (RBC) transfusion is common, but how much is too much? And could transfusion thresholds influence neurologic recovery?
A new systematic review and meta-analysis published in Critical Care Medicine by Larcipretti et al. (2025) has brought compelling insights into this debate, potentially reshaping current transfusion guidelines for TBI management.
Study overview
Objective:
To compare liberal vs. restrictive transfusion strategies in TBI patients with respect to safety and neurologic outcomes.
Design:
- Meta-analysis of 5 randomized controlled trials
- Total participants: 1,533 patients
- Split: 769 (liberal strategy), 764 (restrictive strategy)
Primary endpoint:
Favorable Glasgow Outcome Scale (GOS) scores at 6 months post-TBI.
Secondary endpoints:
- ICU and hospital mortality
- Infection and thromboembolic events
- Length of hospital stay (LOS)
- Transfusion-related complications
What are the transfusion strategies?
1. Restrictive strategy
- Hemoglobin threshold: < 7 g/dL
- Fewer blood units transfused
- Supported by past guidelines (TRICC trial, Cochrane reviews)
2. Liberal strategy
- Hemoglobin threshold: ≥ 9–10 g/dL
- Aims to prevent cerebral hypoxia and ischemia
- More common in TBI-specific clinical settings
Major findings
Neurologic outcomes
- Favorable outcomes were slightly higher with liberal transfusion.
- Leave-one-out sensitivity analysis showed statistical significance when one outlier study was excluded.
Mortality
- No difference in:
- Hospital mortality
- ICU mortality
- Follow-up mortality
Transfusion volume
- Liberal group received 2.92 more units of RBCs on average.
Complications
- ARDS significantly more frequent in the liberal group.
- No significant difference in infections or thromboembolic events.
Length of stay
- No notable difference in ICU or hospital stay durations.
Clinical implications
- The current restrictive transfusion guidelines, based largely on general critical care populations, may not adequately support TBI recovery.
- Neurologic recovery—not just survival—should be a primary consideration in transfusion decisions.
- Future research should focus on defining the optimal balance between oxygen delivery and transfusion risks in TBI.
Conclusion
This new study is a landmark in transfusion research for traumatic brain injury. It suggests that we may need to move beyond one-size-fits-all strategies and start tailoring hemoglobin thresholds to specific clinical situations.
“Better brains need better blood—but not at the cost of breath.”
With growing evidence in support of the 9 g/dL hemoglobin threshold, it may be time for clinicians and policymakers to revise current transfusion protocols and give TBI patients the best shot at recovery.
Reference: Larcipretti et al., Transfusion Practices in Traumatic Brain Injury, Critical Care Medicine 2025; 53: e963-e972.
For more information on TBI and transfusion protocols, check out Anesthesia Updates on the NYSORA Anesthesia Assistant App.
Get access to step-by-step management algorithms, the latest research, and peer-reviewed insights—all in one place. Download the app today and experience the future of anesthesia education and decision-making.