
 Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Definition of placenta accreta spectrum
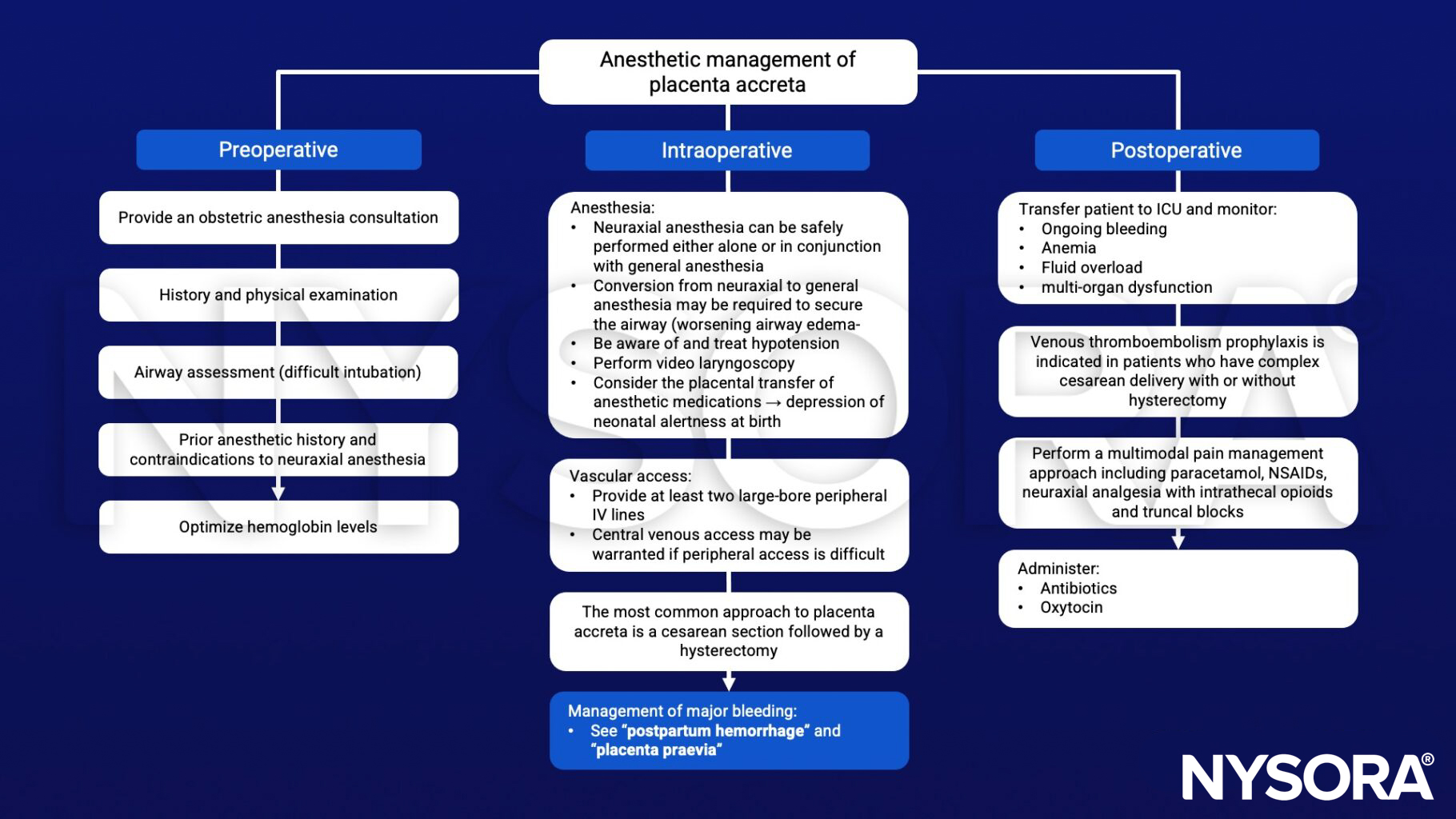
- Anesthetic management of placenta accreta
Definition and mechanisms
- Refers to a severe pregnancy complication that occurs when the placenta grows too deeply into the uterine wall
- With placenta accreta, part or all of the placenta remains attached after delivery, thereby possibly leading to severe blood loss after delivery
- Is considered a high-risk pregnancy complication
- Three types:
- Placenta accreta:
- Placental villi adhere to the myometrium
- Placenta does not pass through the wall of the uterus and does not impact the uterine muscles
- Majority of cases
- Placenta increta:
- Invasion of the myometrium
- Placenta does not pass through the uterine wall
- 15-18% of cases
- Placenta percreta:
- Invasion through the myometrium to the serosa and surrounding organs
- Might impact other organs such as the bladder or intestines
- Most severe
- 5-7% of cases
- Placenta accreta:
Signs and symptoms
- Often no signs or symptoms
- Although vaginal bleeding during the third trimester might occurs
Risk factors
- Previous uterine surgery or caesarean section
- Placenta position: if the placenta partially or totally covers the cervix (placenta previa) or sits in the lower portion of the uterus
- Maternal age > 35 years
- Multiparity
- IVF
Complications
- Major vaginal bleeding
- Thromboembolism
- Coagulopathy
- Anemia
- Premature birth
- Amniotic fluid embolism
- Damage to the uterus and surrounding organs
- Loss of fertility due to a hysterectomy
- Acute transfusion reaction
- Acute respiratory distress syndrome (ARDS)
- Acute kidney injury
- Infection
- Multisystem organ failure
Diagnosis
- Ultrasound
- MRI
Management
- Planning for delivery
- Obstetricians will plan delivery between 35+0 and 36+6 weeks gestation in women stringy suspected to have placenta accreta
- Administer a single course of antenatal glucocorticoids between 34 and 36 weeks of gestation
- Symptoms of bleeding or preterm labor may hasten the need for delivery
Suggested reading
- Reale, S.C., Farber, M.K., 2022. Management of patients with suspected placenta accreta spectrum. BJA Education 22, 43–51.
- Silver RM, Barbour KD. Placenta accreta spectrum: accreta, increta, and percreta. Obstet Gynecol Clin North Am. 2015;42(2):381-402.
Clinical updates
Azem et al. (2025, EJA) report real-world outcomes for placenta accreta spectrum cases managed with planned REBOA (Zone 3) across four centers: neuraxial anesthesia was used initially in 85%, but over half (52.5%) required conversion to general anesthesia, most often for breakthrough pain and surgeon request. Ultrasound-guided REBOA placement was associated with a markedly shorter anesthesia-to-delivery interval than fluoroscopy (median 60 vs 111 minutes), and balloon inflation was avoided in ~23% after intraoperative assessment, supporting selective rather than automatic use.
Padilla et al. (Anesthesiology, 2026) report in a large multicenter cohort that the most common anesthetic approach for placenta accreta spectrum cesarean hysterectomy is neuraxial anesthesia with conversion to general anesthesia, followed by general anesthesia alone and neuraxial alone, with increasing use of neuraxial-only techniques over time. More severe disease, unscheduled cases, and higher ASA status significantly increased the likelihood of choosing general anesthesia, while institutional practice accounted for substantial variability in anesthetic choice.
- Read more about this study HERE.











