
 Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Definition of transurethral resection of the prostate (TURP) syndrome
- Management of TURP
Definition and mechanisms
- Benign prostatic hyperplasia (BPH) occurs in over
- 40% of men aged over 60 years and prostate resection is the second-line treatment if BPH symptoms are resistant to medical management
- Transurethral resection of the prostate (TURP) syndrome is a rare but potentially life-threatening complication of transurethral resection of the prostate procedure
- During the procedure, the prostate at the bladder neck is shaved away
- As the body of the prostate is removed, veins are exposed, but the capsule is maintained
- The exposed veins can bleed, causing significant blood loss, and can also absorb large amounts of irrigation fluid resulting (1.5% glycine solution) in TURP syndrome
- Treatment is largely supportive and relies on the removal of the underlying cause and organ and physiological support
- Mortality is 0.2-0.8%
- Pre-operative prevention strategies are extremely important
Signs and symptoms
- Signs and symptoms are often vague and non-specific as there is no classical TURP presentation
- Symptoms result from fluid overload and disturbed electrolyte balance, and hyponatremia
Central nervous system Restlessness
Headache
Nausea and vomiting
Confusion
Visual disturbances
Cerebral edema
Seizures
Coma
Cardio-respiratory Bradycardia
Hypotension or Hypertension
Tachypnea
Hypoxia
Cyanosis
Pulmonary edema
Systemic Hypothermia
Abdominal pain and distension
Complications of TURP procedure
- Retrograde ejaculation
- Urinary incontinence
- Erectile dysfunction
- Urethral strictures (narrowing of the urethra)
- Bleeding
- Urinary tract infection
- Urinary retention
Risk factors
- The size of the opened venous sinuses
- The amount of irrigation fluid used
- The use of excess amounts of hypotonic intravenous fluids
- Duration of the resection (> 1 hour)
- Perforation of the bladder
Diagnosis
- Acutely unwell, confused patient with a reduced Glasgow Coma Scale score
- Hyponatremia: Na < 120 mmol/L
- Hyperkalemia: K > 6.0 mml/L
- Glycine toxicity
- Intravascular hemolysis
- Disseminated intravascular coagulation
Prevention
- Regional anesthesia is preferred over general anesthesia
- Avoid large amounts of glycine-containing fluid infusion
- Keep the length of surgery under 1 hour
- Keep the patient horizontal and avoid the Trendelenburg position
- Resect large prostates in staged procedures to avoid prolonged operative times
- The optimal height of the irrigation fluid bag above the patient is 60 cm
Management
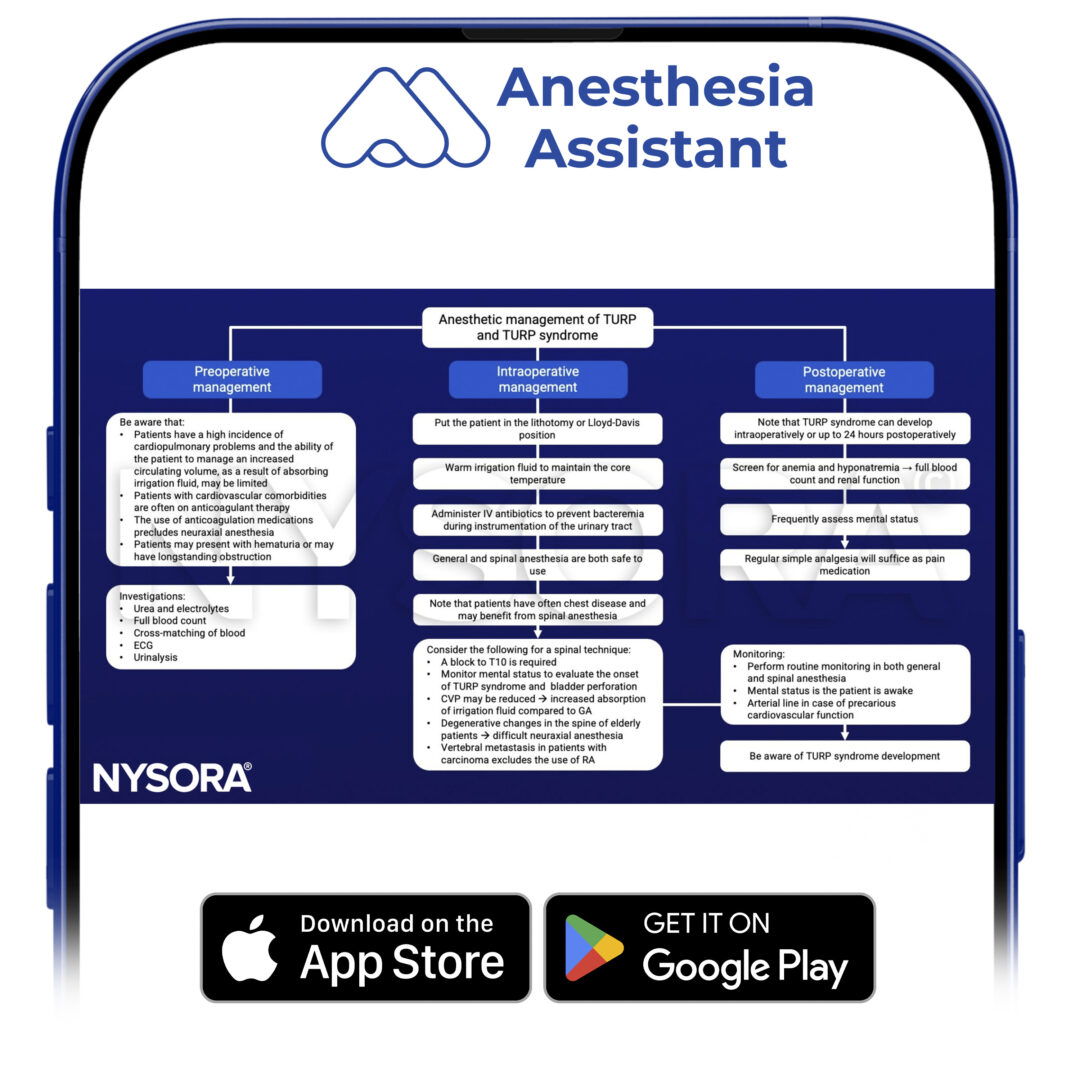
From diagnosis to recovery.
Have TURP guidance instantly available.
Treatment of TURP syndrome
- Stop the procedure as soon as possible
- Provide oxygenation (intubation) & circulatory support (inotropes)
- Perform invasive monitoring if hemodynamically unstable
- Treat hypotension
- Correct hyponatremia
- Treat fluid overload with diuretics
- Manage disseminated intravascular coagulation
- Perform regular blood tests to monitor improvement in the clotting status
- Control seizures with benzodiazepines
- Treat nausea and vomiting with antiemetics
Suggested reading
- Pollard BJ, Kitchen, G. Handbook of Clinical Anaesthesia. Fourth Edition. CRC Press. 2018. 978-1-4987-6289-2.
- Nakahira, J., Sawai, T., Fujiwara, A., Minami, T., 2014. Transurethral resection syndrome in elderly patients: a retrospective observational study. BMC Anesthesiology 14, 30.
- Demirel I, Ozer AB, Bayar MK, Erhan OL. TURP syndrome and severe hyponatremia under general anaesthesia. BMJ Case Rep. 2012;2012:bcr-2012-006899.
- O’Donnell AM, Foo I. 2009. Anaesthesia for transurethral resection of the prostate. Continuing Education in Anaesthesia Critical Care & Pain. 9;3:92-96.











