Learning objectives
- Describe scleroderma
- Recognize the symptoms and signs of scleroderma
- Anesthetic management of a patient with scleroderma
Definition and mechanisms
- Scleroderma or systemic sclerosis (SSc) is a systemic, immune-mediated disease characterized by abnormal cutaneous and organ-based fibrosis, resulting in hardening and tightening of the skin, and progressive end-organ dysfunction
- SSc is characterized by increased synthesis of collagen (leading to sclerosis), damage to small blood vessels, activation of T lymphocytes, and production of altered connective tissue
Signs, symptoms, and complications
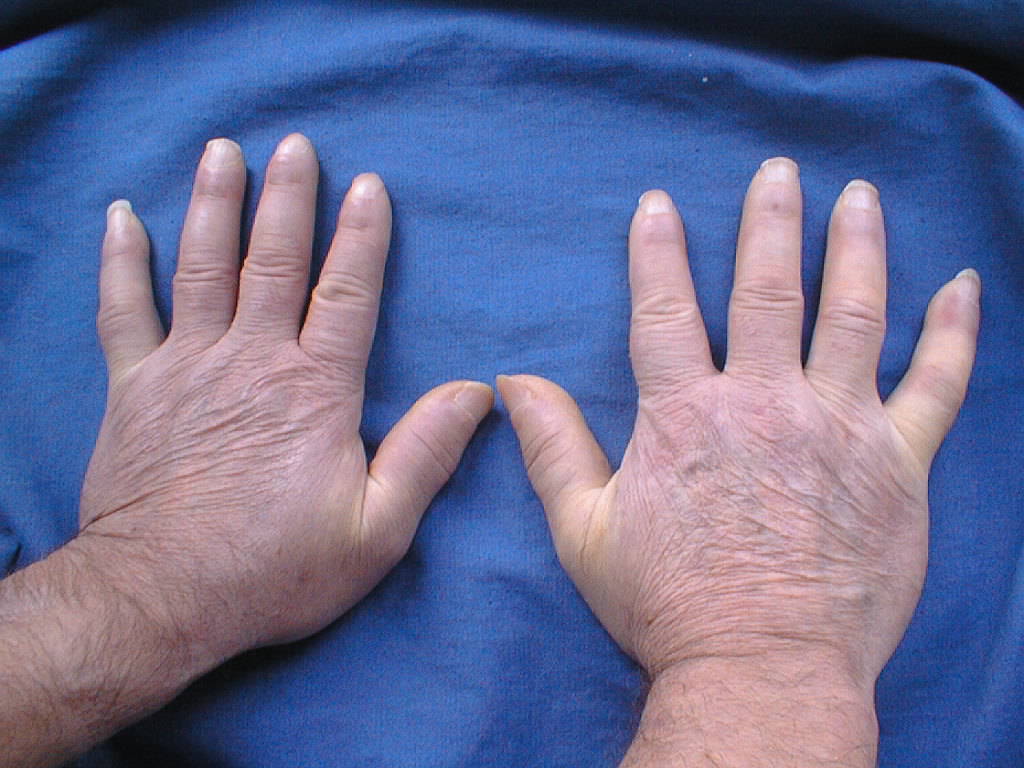
- Cardiovascular: Raynaud’s phenomenon, healed pitting ulcers on the fingertips, skin and mucosal telangiectasis, palpitations, irregular heart rate, and fainting due to conduction abnormalities, hypertension, and congestive heart failure (CHD)
- Pulmonary: Progressive worsening of dyspnea, chest pain (due to pulmonary hypertension), and dry, persistent cough due to interstitial lung disease (ILD)
- Digestive: Gastroesophageal reflux disease (GERD), bloating, indigestion, loss of appetite, diarrhea alternating with constipation, sicca syndrome and its complications, loosening of teeth, and hoarseness (due to acid reflux)
- Musculoskeletal: Joint, muscle aches, loss of joint range of motion, carpal tunnel syndrome, calcinosis, and weight loss
- Genitourinary: Erectile dysfunction, kidney failure
- Other: Facial pain due to trigeminal neuralgia, hand paresthesias, headache, stroke, and fatigue
Risk factors
- Family history
- Certain genetic factors
- Gender: Occurs more in women than in men
- Exposure to silica, viruses, medications, and drugs
Treatment
There is no treatment that can cure or stop the overproduction of collagen, which is characteristic of SSc. Treatment mainly focuses on controlling symptoms and preventing complications.
- Raynaud’s phenomenon: Vasodilators (e.g., calcium channel blockers, α-blockers, serotonin receptor antagonists, angiotensin II receptor inhibitors, statins, local nitrates, or iloprost)
- Digital ulcers: Phosphodiesterase-5-inhibitors or iloprost
- Prevention of new digital ulcers: Bosentan
- Malnutrition: Tetracycline antibiotics
- Interstitial lung disease: Cyclophosphamide, azathioprine with or without corticosteroids
- Pulmonary arterial hypertension: Endothelin receptor antagonists, phosphodiesterase-5-inhibitors, and prostanoids
- Gastroesophageal reflux disease: Antacids or prokinetics
- Kidney crises: Angiotensin-converting enzyme inhibitors and angiotensin II receptor antagonists
Management
Preoperative risk identification and stratification
- Airway
- Microstomia
- Limited cervical extension
- Neurological
- Peripheral neuropathies (paresthesias, numbness)
- Autonomic dysfunction risk factors (orthostatic hypotension)
- Pulmonary hypertension risk factors (dyspnea, increased PASP, RVSP)
- Progressive cardiomyopathy (TTE)
- Conduction abnormalities (ECG)
- ILD risk factors
- DLCO <50%
- CRP ≥5 or ESR ≥20
- Decreased 6-minute walk test
- Sleep-disordered breathing risk (apnea, daytime somnolence)
- STOP-Bang questionnaire
- Sleep study findings
- Esophageal dilation: GERD symptoms
- Malnutrition
- Pseudo-obstruction
- Presence of sarcopenia
- Venous thromboembolic disease risk factors
- SSc diagnosis <12 months
- Atrial fibrillation
- CHD
- Anemia: Preoperative complete blood count
Intraoperative risk mitigation
- Difficult airway preparedness
- Aspiration chemoprophylaxis
- Appropriate padding and positioning
- Availability of ultrasound for difficult intravenous access
- Cardiac monitoring: Arterial line, possible TEE, PA catheter
- Lung protective ventilation strategy
- Minimize adverse drug interactions
- Ensure adequate prophylactic anticoagulation
Postoperative complication surveillance
- Sleep-disordered breathing: Continuous postoperative pulse oximetry
- Increased myocardial infarction: Continuous postoperative telemetry
- ILD deterioration: Presence of increased oxygen requirements >24 hrs after surgery; consider early workup for postoperative pneumonia or exacerbation of ILD
- Venous thromboembolic disease: Surveillance in surgery, trauma, and those administered glucocorticoids
- SSc renal crisis: Refractory HTN, encephalopathy, CHF
Keep in mind
- Patients with SSc often have well-compensated mechanisms for their underlying disease, which may be unmasked with anesthetic interventions
- Anticipate a difficult airway and the potential risk of aspiration
- SSc patients are at risk for postoperative myocardial infarction, and prolonged mechanical ventilation may result in substantial morbidity, specifically in patients with interstitial lung disease
Suggested reading
- Carr ZJ, Klick J, McDowell BJ, Charchaflieh JG, Karamchandani K. An Update on Systemic Sclerosis and its Perioperative Management. Curr Anesthesiol Rep. 2020;10:512-521.