Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Describe porphyria
- Recognize the symptoms and signs of porphyria
- Anesthetic management of a patient with porphyria
Definition and mechanisms
- Porphyrias are a heterogeneous group of inherited genetic disorders of heme biosynthesis
- The heme biosynthetic pathway is most active in the liver and bone marrow
- Porphyrins are organic cyclical compounds found in heme, the iron-containing ring structure found in hemoglobin, myoglobin, and all of the cytochromes
Classification
- Acute porphyrias: Potential to develop acute neurovisceral crises
- Acute intermittent porphyria (AIP)
- Variegate porphyria (VP)
- Hereditary coproporphyria (HCP)
- 5-aminolaevulinic acid (ALA) dehydrase deficiency
- Triggers for an acute crisis
- Fasting
- Dehydration
- Infection
- Drugs
- Endogenous hormones
- Stress
- Smoking
- Alcohol
- Non-acute: Do not deteriorate into acute crises, less relevant for anesthesiologists
- Porphyria cutanea tarda
- Congenital erythropoietic porphyria
- Erythropoietic protoporphyria
Signs and symptoms
Presentation of an acute crisis
- Almost all patients have severe abdominal pain, usually associated with tachycardia
- Symptoms and signs of acute crises vary greatly and can mimic other conditions
| Symptoms and signs | Features | May be misdiagnosed as |
|---|---|---|
| Abdominal pain | Recurrent, severe, poorly localized Associated nausea and vomiting Absence of fever or leucocytosis | Another cause of acute abdomen Endometriosis/pelvic inflammatory disease Irritable bowel syndrome Opiate addiction |
| Cardiovascular signs | Tachycardia Tachyarrhythmia Hypertension | |
| Weakness | Proximal > distal Upper limbs > lower Up to 20% develop respiratory failure May progress to bulbar paresis in severe cases | Guillain-Barré syndrome Poliomyelitis Acute lead poisoning Vasculitis |
| Psychiatric features | Mood disturbance Confusion Psychosis | Anxiety disorder Somatization disorder Acute psychosis Acute confusional state |
| Pain and sensory disturbance | Back, thigh, or extremity pain Sensory neuropathy over the trunk | Chronic fatigue syndrome Fibromyalgia Chronic pain syndromes |
| Seizures | CNS manifestation of porphyria Secondary to hyponatremia | Epilepsy |
| Other autonomic features | Constipation Gastoparesis Postural hypotension | |
| Cutaneous lesions | Only in VP and HCP Vesicular rash Photosensitivity | Porphyria cutanea tarda Bullous skin disease |
| Hyponatremia and other electrolyte disturbance | Low serum sodium Low serum magnesium | Other disorders of sodium and water balance |
Risk factors
- Women are 4 to 5 times more likely to develop crises in their early thirties
Pathophysiology

Treatment
Once an acute crisis has been diagnosed, management consists of the following:
- Remove or treat potential triggering factors and avoid a catabolic state
- Administration of i.v. heme arginate 3 mg/kg daily for 4 days
- Supportive measures
- May require large doses of morphine to control pain
- Antiemetics prochlorperazine and ondansetron are safe
- Control tachycardia and hypertension with β-blockers
- Avoid seizures via correcting hyponatremia and treating with gabapentin, vigabatrin, or levetiracetam
- Sedation with propofol and alfentanil is safe
Management
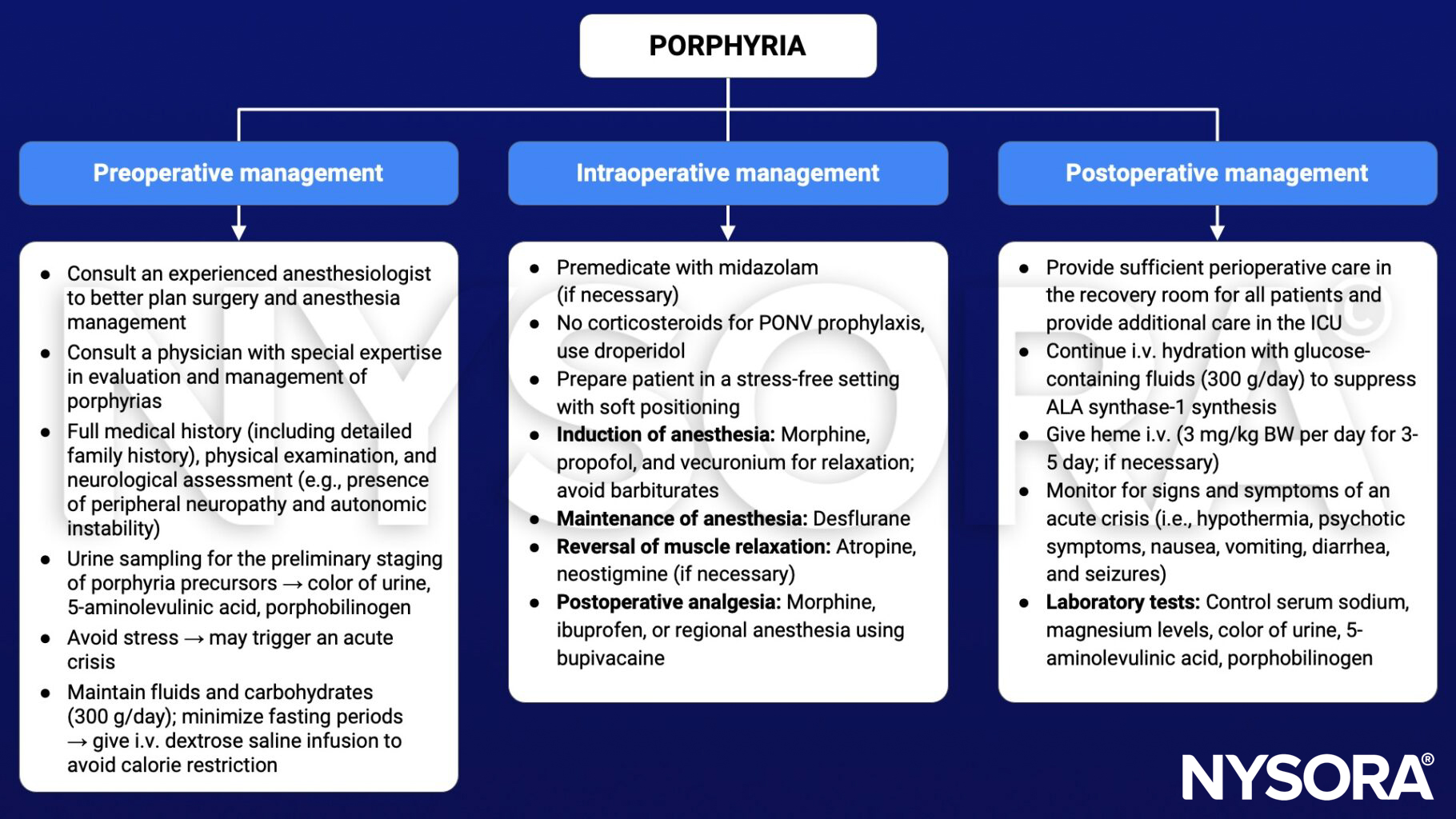
Commonly used drugs and their safety profile
| Drug | Safe | Unsafe | Undetermined |
|---|---|---|---|
| I.v. anesthetic agents | Propofol | Thiopentone, ketamine | Etomidate |
| Inhalational anesthetic agents | Isoflurane, desflurane, nitrous oxide | Sevoflurane | |
| Local anesthetics | Bupivacaine, prilocaine, lidocaine | Levobupivacaine, ropivacaine | |
| Neuromuscular blocking agents and removal | Succinylcholine, all non-depolarizing muscle relaxants, neostigmine | ||
| Analgesics | Fentanyl, alfentanil, remifentanil, morphine, hydromorphone, meperidine, tramadol, ibuprofen, aspirin | Oxycodone, diclofenac | Pentazocine, mefenamic acid |
| Sedative premedication | Lorazepam, phenothiazines (chlorpromazine), temazepam | ||
| Antibiotics | Gentamicin, co-amoxiclav, penicillins, vancomycin, tazocin, meropenem | Rifampicin, erythromycin | |
| Cardiovascular drugs | Adrenaline, noradrenaline, milrinone, atropine, glycopyrrolate, β-blockers, phenylephrine, magnesium, angiotensin 2 inhibitors, fibrinolytic drugs | Ephedrine | Vasopressin, metaraminol |
| Miscellaneous | Syntocin, carboprost, tranexamic acid, aprotinin | Dexamethasone, hydrocortisone |
Keep in mind
- Anesthesiologists should be aware of the perioperative factors that may trigger or worsen an acute crisis in porphyria
Suggested reading
- Findley H, Philips A, Cole D, Nair A. Porphyrias: implications for anaesthesia, critical care, and pain medicine. Continuing Education in Anaesthesia Critical Care & Pain. 2012;12(3):128-133.