
 Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About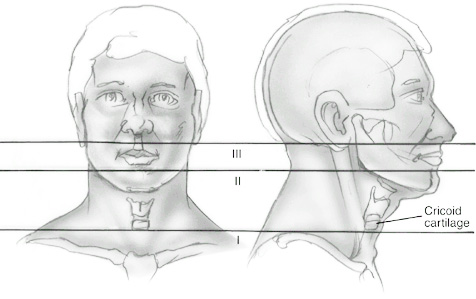
Learning objectives
- Recognize penetrating neck injuries
- Management of penetrating neck injuries
Definition and mechanism
- Trauma to the neck by breaching the platysma muscle
- Caused by stab wounds, gunshot wounds, self-harm, road traffic accidents, and other high-velocity objects
- Partial or complete occlusion, dissection, pseudoaneurysm, extravasation of blood, or arteriovenous fistula formation
- Potential for serious & life-threatening injuries
- Laryngeal/tracheobronchial tree disruption
- Tension/open pneumothorax, massive hemothorax
- Major vascular disruption
- Esophageal tear
- Spinal cord injury, nerve injury
Signs and symptoms
- Shock
- Active hemorrhage
- Pulsatile bleeding or expanding hematoma
- Audible bruit or papable thrill
- Airway compromise
- Wound bubbling
- Subcutaneous emphysema
- Stridor
- Hoarseness
- Difficulty/pain when swallowing
- Hemiparesis
- Neurological deficits
Anatomical zones of penetrating neck injury
| Zone | Anatomical boundaries | Anatomical structures at risk |
|---|---|---|
| 1 | Superior boundary: skull base Inferior boundary: angle of the mandible | Pharynx Carotid arteries Internal jugular veins Cranial nerves Sympathetic chain Parotid gland |
| 2 | Superior boundary: angle of the mandible Inferior boundary: cricoid cartilage | Laryngotracheal complex Pharynx Oesophagus Carotid artery Jugular veins Vertebral arteries Spinal cord Vagus and phrenic nerves |
| 3 | Superior boundary: cricoid cartilage Inferior boundary: clavicles | Trachea Oesophagus Carotid artery Jugular veins Thoracic duct Spinal cord Cranial nerves Vertebral arteries |
Management
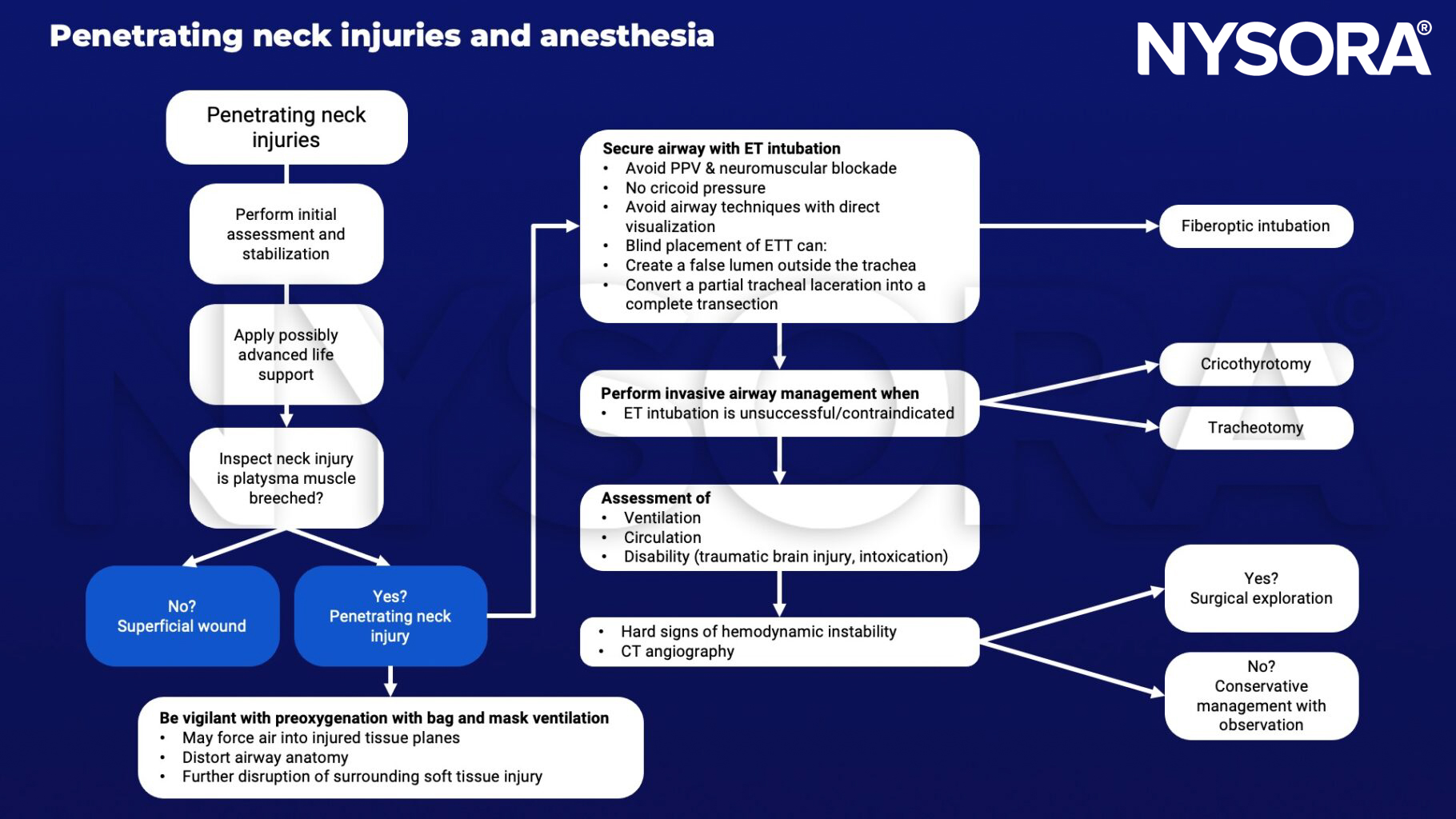
Keep in mind
- Full stomach/RSI vs potentially challenging airway
- Uncooperative patient vs. awake fiberoptic bronchoscopic intubation
- Securing airway vs. consequences of PPV
Suggested reading
- McCann C, Watson A, Barnes D. Major burns: Part 1. Epidemiology, pathophysiology and initial management. BJA Educ. 2022;22(3):94-103.
- Nowicki JL, Stew B, Ooi E. Penetrating neck injuries: a guide to evaluation and management. Ann R Coll Surg Engl. 2018;100(1):6-11.
- Huh H, Han JH, Chung JY, et al. Anesthetic management of penetrating neck injury patient with embedded knife -A case report-. Korean J Anesthesiol. 2012;62(2):172-174.
Clinical updates
Kristensen et al. (Current Opinion in Anesthesiology, 2025) emphasize that airway threats seen in penetrating neck injuries, distorted anatomy, bleeding, edema, and shared surgical airways mirror those in complex head and neck surgery, making early risk stratification and awake tracheal intubation critical when obstruction or failed ventilation is anticipated. The review highlights awake flexible bronchoscopic or video-assisted techniques as safest in unstable or anatomically compromised necks, with immediate preparedness for front-of-neck access (cricothyrotomy or tracheostomy) to mitigate rapid loss of airway control. Video laryngoscopy is recommended as first-line when anatomy permits, but only with clearly defined backup plans and close surgical collaboration.
- Read more about this study HERE.












