Learning objectives
- Describe the pathophysiology of metabolic alkalosis
- Diagnose metabolic alkalosis
- Manage metabolic alkalosis
Background
- Metabolic alkalosis is defined as an increase in serum pH to >7.45
- Mostly due to a primary increase in serum bicarbonate (HCO3-)
- Associated with a secondary increase in CO2 arterial pressure (PaCO2)
- Usually accompanied by hypokalemia and hypochloremia
- Common aced-base disorder in critically ill patients
Pathophysiology
- Intracellular shift of hydrogen ions
- E.g. hypokalemia
- Decrease in serum hydrogen ions results in a relative increase in bicarbonate
- Renal loss of hydrogen ions
- Pathologies that increase the levels of mineralocorticoids or the effect of aldosterone lead to hypernatremia, hypokalemia, and hydrogen loss
- Loop and thiazide diuretics can induce secondary hyperaldosteronism
- Genetic defects leading to decreased expression of ion transporters in the loop of Henle (Bartter disease, Gitelman disease)
- Retention/addition of bicarbonate
- Overdose of exogenous sodium bicarbonate
- Compensatory mechanism for hypercarbia: hypoventilation and CO2 retention result in renal compensation over time by retaining bicarbonate (post-hypercapnia syndrome)
- Contraction alkalosis
- Occurs when a large volume of sodium-rich, bicarbonate low fluid is lost
- Diuretic use, cystic fibrosis, congenital chloride diarrhea
- Net concentration of bicarbonate increases
- Evaluation of etiology: Urinary chloride
- Chloride responsive (urine chloride <10 mEq/L): Gastrointestinal hydrogen loss, congenital chloride diarrhea syndrome, contraction alkalosis, diuretic therapy, post-hypercapnia syndrome, cystic fibrosis, exogenous alkalotic agent use, villous adenoma, high volume ileostomy output
- Chloride resistant (urine chloride >20 mEq/L): Retention of bicarbonate, intracellular shift of hydrogen, hyperaldosteronism, Bartter syndrome, Gitelman syndrome, Cushing’s syndrome, exogenous mineralocorticoids, congenital adrenal hyperplasia, licorice, Liddle syndrome
- Adverse effects
- Decreased myocardial contractility
- Arrhythmias
- Decreased cerebral blood flow
- Delirium
- Increased neuromuscular excitability
- Impaired peripheral oxygen unloading
- Compensatory increase in arterial pCO2
- Net effect resulting in hypoxia
Diagnosis
- Elevated serum HCO3- and pCO2
- Determine respiratory compensation
- PaCO2 (mmHg) = 40 + 0.6 × (HCO3- – 24 mmol/l)
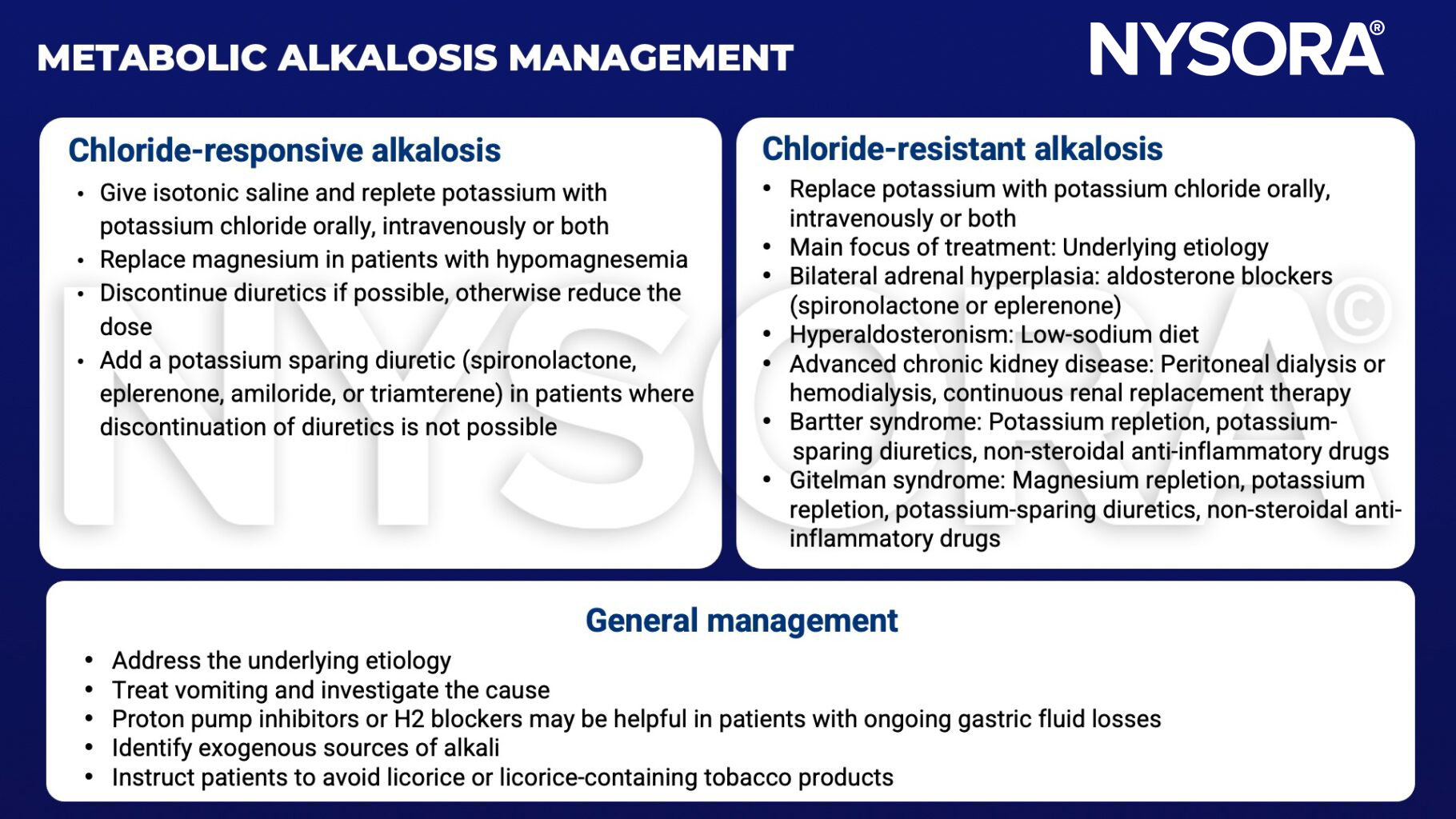
Management
Suggested reading
- Brinkman JE, Sharma S. Physiology, Metabolic Alkalosis. [Updated 2022 Jul 18]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK482291/
- Tinawi M. Pathophysiology, Evaluation, and Management of Metabolic Alkalosis. Cureus. 2021;13(1):e12841. Published 2021 Jan 21.
Clinical updates
Coppola et al. (2025, BJA) highlight that loop and thiazide diuretics are major, often underappreciated drivers of metabolic alkalosis in critically ill patients, through volume depletion, hypochloremia, and increased distal hydrogen ion secretion. The review emphasizes acetazolamide as a targeted adjunct to correct diuretic-induced metabolic alkalosis by promoting renal bicarbonate loss, particularly in ventilated patients where alkalosis may impair CO₂ clearance and delay weaning.
- Read more about this study HERE.