

Learning objectives
- Definition of sepsis
- Diagnostic features of sepsis
- Management of sepsis
Definition and mechanisms
- Sepsis is a dysregulated systemic response to infection that is associated with organ dysfunction
- Quick sequential organ failure assessment (qSOFA) criteria:
- Altered mental status (GCS score < 15)
- Systolic blood pressure < 100 mmHg
- Respiratory rate > 22 breaths per min
- Septic shock is defined as low blood pressure due to sepsis that does not improve after fluid replacement
- Characterized by high morbidity and mortality (30-50% of affected patients)
- Septic patients are at risk for secondary injuries
- Bacteria, fungi, and viruses can all cause sepsis
Signs and symptoms
- Fever or hypothermia
- Increased heart rate
- Increased breathing rate
- Confusion
- Hypotension
- Sweating
- Edema
- Low urine output
Risk factors
- People older than 65 years old, newborns and infants, and pregnant people
- Medical conditions such as diabetes, obesity, cancer, and kidney disease
- A weakened immune system
- People who are in the hospital for other medical reasons
- Severe injuries, such as large burns or wounds
- Patients with catheters, IVs, or breathing tubes
Diagnostic features
| Organ system | Alteration of dysfunction |
|---|---|
| Neurological | Delirium Altered mental status Ischemia Formation of blood clots in small blood vessels Microabscesses Multifocal necrotizing leukoencephalopathy |
| Cardiovascular | Vasodilation Hypovolemia Cardiac dysfunction Systolic and diastolic dysfunction |
| Pulmonary | Tachypnea Poor gas exchange Acute Respiratory Distress Syndrome |
| Gastrointestinal | Ileus Hyperbilirubinemia |
| Kidney | Oliguria Elevated plasma urea and creatinine Volume overload |
| Hepatic | Disruption of blood clotting Elevated unconjugated serum bilirubin levels |
| Hematological | Perioperative anemia Thrombocytopenia Coagulopathy Disseminated Intravascular Coagulation (DIC) |
| Endocrine and metabolic | Hyperglycemia Sick euthyroid syndrome Elevated lactate |
| Infectious disease | Leucocytosis Elevated inflammatory mediators |
Treatment
- Aggressive source control, resuscitation, and antibiotic therapy are the mainstays of management
- Be aware of subtle changes such as hyperglycemia, ileus, mental status changes, and potential sources of infections

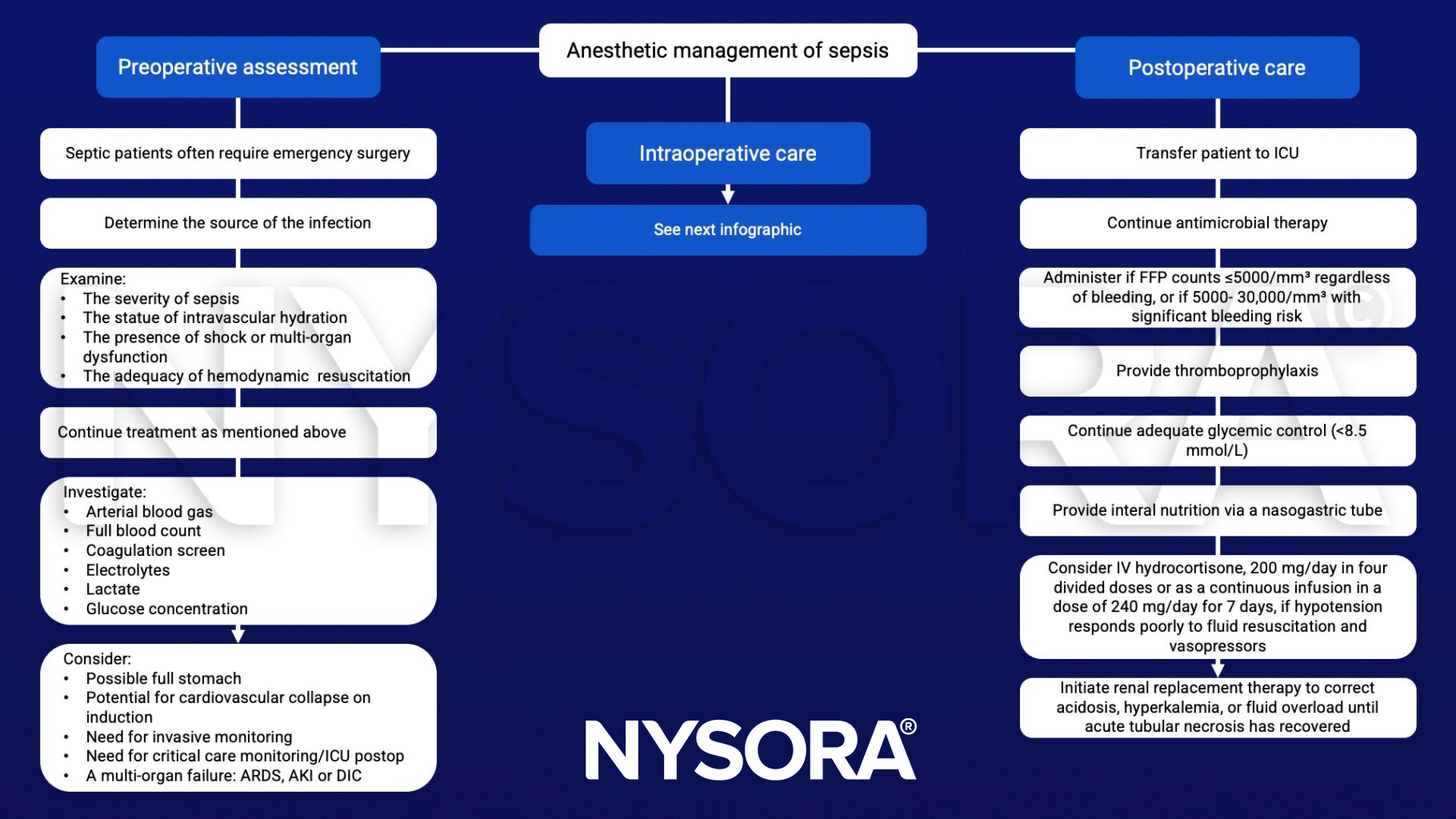
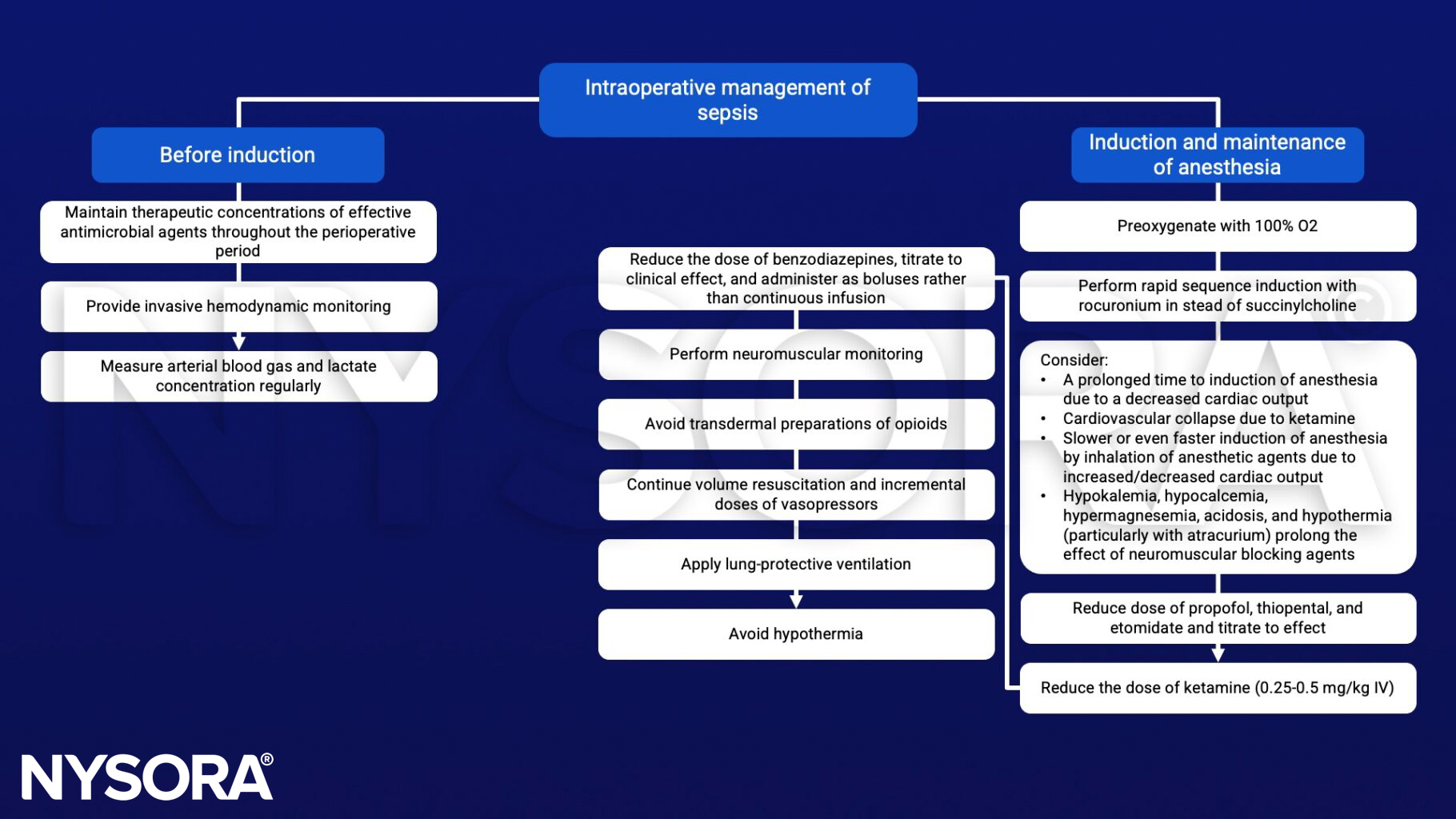
Anesthetic management
Suggested reading
- Ammar, M.A., Ammar, A.A., Wieruszewski, P.M. et al. Timing of vasoactive agents and corticosteroid initiation in septic shock. Ann. Intensive Care 12, 47 (2022).
- Charlton, M., Thompson, J.P., 2019. Pharmacokinetics in sepsis. BJA Education 19, 7–13.
- Gyawali B, Ramakrishna K, Dhamoon AS. Sepsis: The evolution in definition, pathophysiology, and management. SAGE Open Med. 2019;7:2050312119835043.
- Keeley A, Hine P, Nsutebu EThe recognition and management of sepsis and septic shock: a guide for non-intensivistsPostgraduate Medical Journal 2017;93:626-634.
- Nunnally, M.E., 2016. Sepsis for the anaesthetist. British Journal of Anaesthesia 117, 44–51.
- Eissa D, Carton EG, Buggy DJ. Anaesthetic management of patients with severe sepsis. Br J Anaesth. 2010;105(6):734-743.
Clinical updates
Antonucci et al. (Anesthesiology, 2024) report that optimal hemodynamic support in sepsis relies on early administration of balanced crystalloids (30 mL/kg), combined with early initiation of norepinephrine to rapidly achieve a MAP ≥ 65 mmHg while avoiding fluid overload. Recent trials have shown no difference in mortality between restrictive and liberal fluid strategies but emphasize dynamic assessment of fluid responsiveness, lactate clearance, and peripheral perfusion, with vasopressin or angiotensin II reserved for refractory vasodilatory shock.
- Read more about this study HERE.












