Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About





Sepsis, a life-threatening organ dysfunction due to a dysregulated host response to infection, requires prompt antimicrobial therapy, source control, and correction of hemodynamic abnormalities. Managing sepsis-induced hemodynamic changes is critical to improving patient outcomes. This review presents evidence-based recommendations for fluid resuscitation, vasopressor use, and hemodynamic targets in adults with sepsis.
Key recommendations for hemodynamic support in sepsis
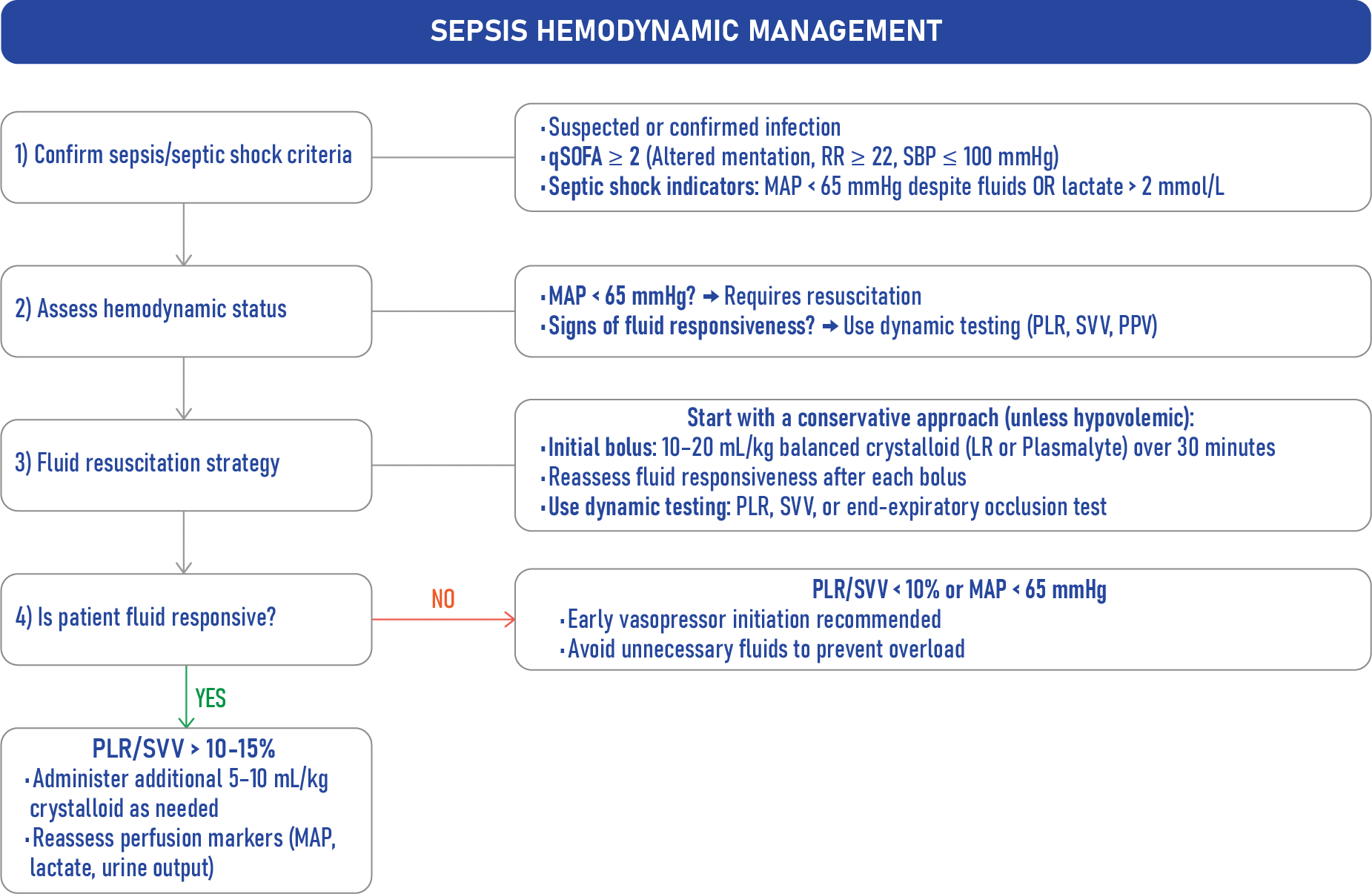
Fluid resuscitation
Initial fluid therapy:
- Administer 30 ml/kg of crystalloids within the first 3 hours of sepsis, based on 2021 Surviving Sepsis Campaign guidelines.
- Tailor fluid administration using hemodynamic monitoring (e.g., echocardiography, dynamic parameters) to avoid overresuscitation.
Restrictive vs. Liberal fluid therapy:
- The CLASSIC trial found no difference in 90-day mortality between restrictive and standard fluid therapy in septic shock.
- The CLOVERS trial showed no mortality difference between restrictive and liberal fluid strategies but noted earlier vasopressor use in the restrictive group.
Fluid responsiveness:
- Approximately 30% of septic shock patients are non-responders to fluids.
- Dynamic tests like passive leg raise and end-expiratory occlusion test predict fluid responsiveness and help limit unnecessary fluid administration.
Choice of fluids
Balanced crystalloids (Lactated Ringer’s, Plasmalyte):
- Preferred over normal saline to reduce the risk of hyperchloremic metabolic acidosis and improve kidney function.
- The SMART trial showed fewer major adverse kidney events and lower mortality in sepsis patients receiving balanced crystalloids.
Albumin:
- Hyper-oncotic albumin may reduce fluid balance but has not shown a significant mortality benefit in sepsis.
- The ALBIOS trial found a mortality reduction in septic shock patients but not in the broader sepsis population.
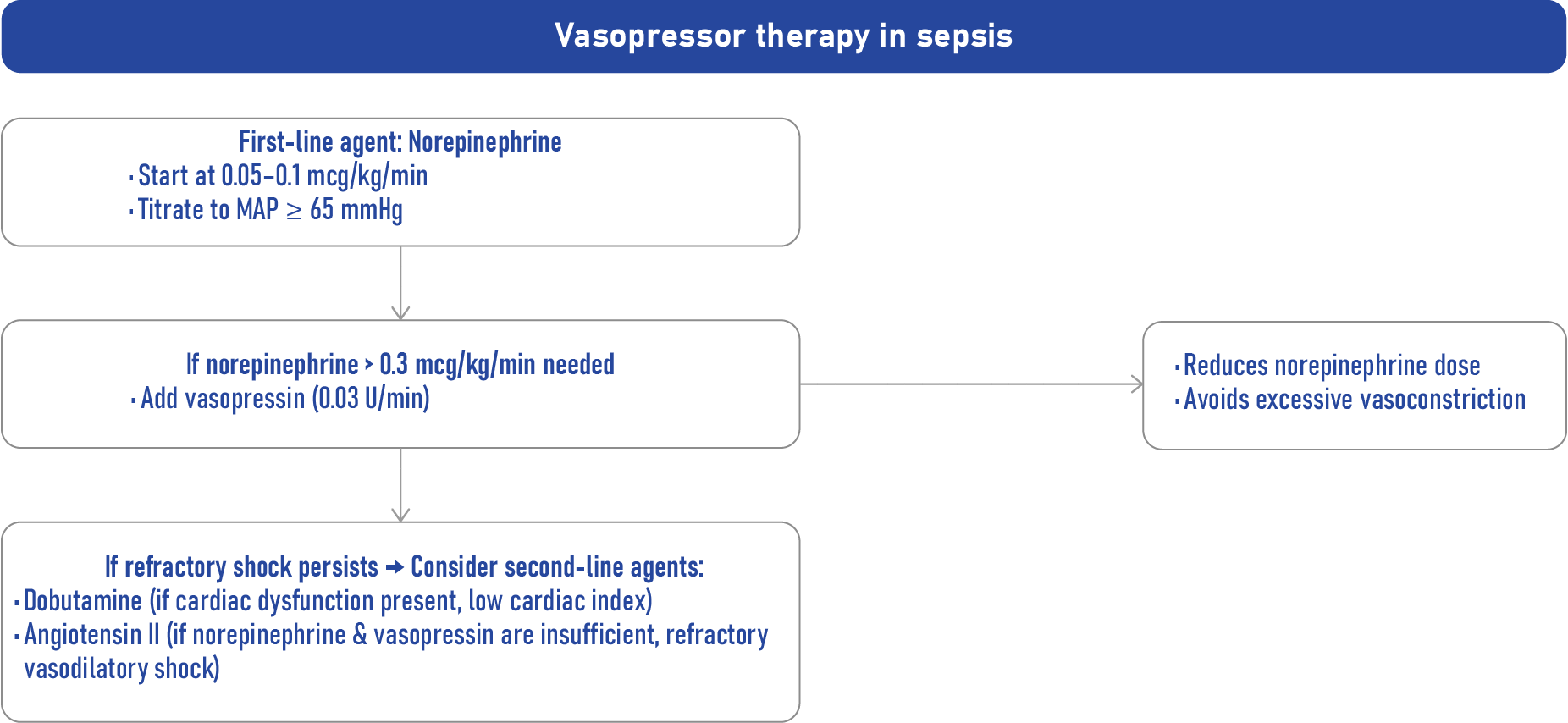
Vasopressor therapy
- When to start:
- Initiate norepinephrine as the first-line vasopressor when MAP < 65 mmHg, even if fluid resuscitation is incomplete.
- Early vasopressor use reduces fluid balance and improves shock control without increasing adverse effects.
- Peripheral vasopressors:
- Safe for short-term use in peripheral veins, with a low risk of local complications.
- Second-line vasopressors:
- Vasopressin: Added to norepinephrine to reduce catecholamine requirements and atrial fibrillation risk.
- Angiotensin II: Considered in refractory vasodilatory shock, especially in patients with AKI or high renin levels.
Monitoring and targets
Mean Arterial Pressure (MAP):
- Target 65-70 mmHg for most patients.
- Higher targets (80-85 mmHg) may benefit patients with chronic hypertension but increase the risk of atrial fibrillation.
Lactate clearance:
- Reducing lactate by ≥20% every 2 hours is associated with lower mortality.
Peripheral perfusion:
- Normalizing capillary refill time is a simple and effective target for resuscitation.
Dynamic assessment of fluid responsiveness
Passive leg raise test:
- Reliable, non-invasive, and independent of breathing effort or tidal volume.
End-expiratory occlusion test:
- Requires mechanical ventilation; useful for detecting fluid responsiveness.
Mini-fluid challenge:
- Rapid infusion of 100 ml fluid to assess stroke volume response.
Conclusion
Optimal hemodynamic support in sepsis involves early fluid resuscitation with balanced crystalloids, timely initiation of norepinephrine, and dynamic assessment of fluid responsiveness to prevent fluid overload. Second-line vasopressors like vasopressin and angiotensin II are reserved for refractory shock. Monitoring MAP, lactate clearance, and peripheral perfusion ensures adequate tissue oxygenation and improves survival. These evidence-based strategies are essential for improving outcomes in patients with sepsis.
For more detailed information, refer to the full guidelines published in Anesthesiology.
Reference: Antonucci E, Garcia B, Legrand M. Hemodynamic Support in Sepsis [published correction appears in Anesthesiology. 2024 Dec 1;141(6):1224-1225. doi: 10.1097/ALN.0000000000005168.]. Anesthesiology. 2024;140(6):1205-1220.
Read about this topic and more on NYSORA’s Anesthesia Assistant App. Don’t miss out—download now.