Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
AboutGoal
Assessment of the function of the left ventricle: normal vs. reduced.
Left ventricle dysfunction may be caused by:
- Coronary artery disease
- Hypertension
- Left ventricular hypertrophy
- Valvular dysfunction
- Myocarditis
Note
This assessment uses a qualitative, not a quantitative, approach. The goal is to identify undifferentiated shock states and tailor management. Note that accurate ejection fraction measurements are reserved for advanced echocardiographers.
Views
Parasternal long-axis view (PLAX)
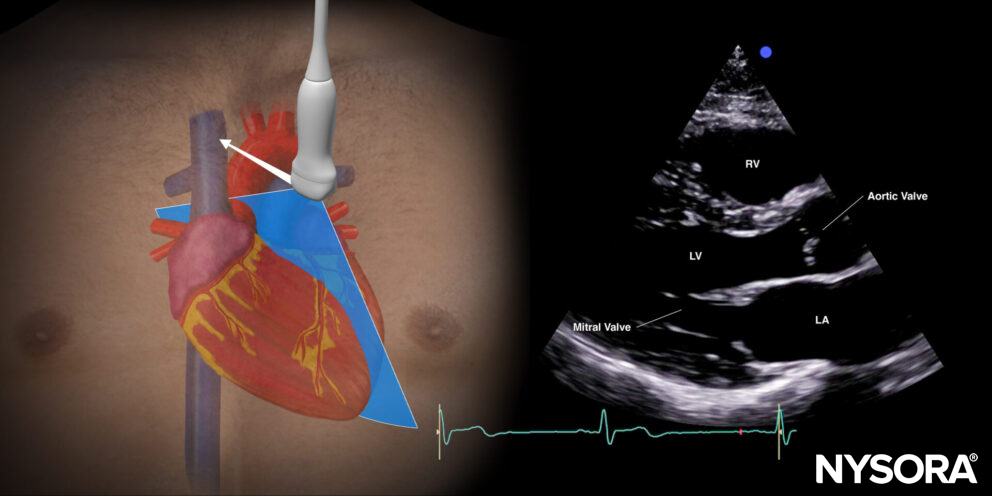
Transducer position and sonoanatomy of the parasternal long-axis view.
Parasternal short-axis view (PSAX)
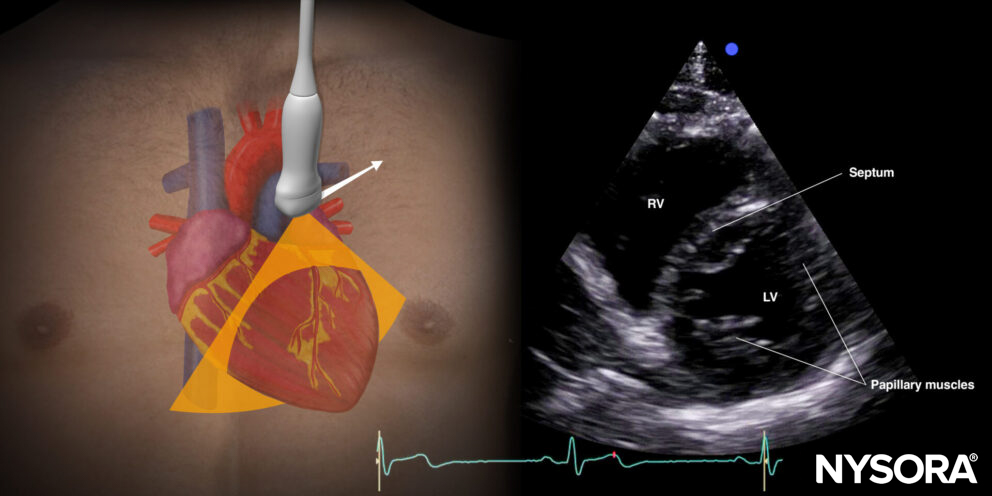
Transducer position and sonoanatomy of the parasternal short-axis view.
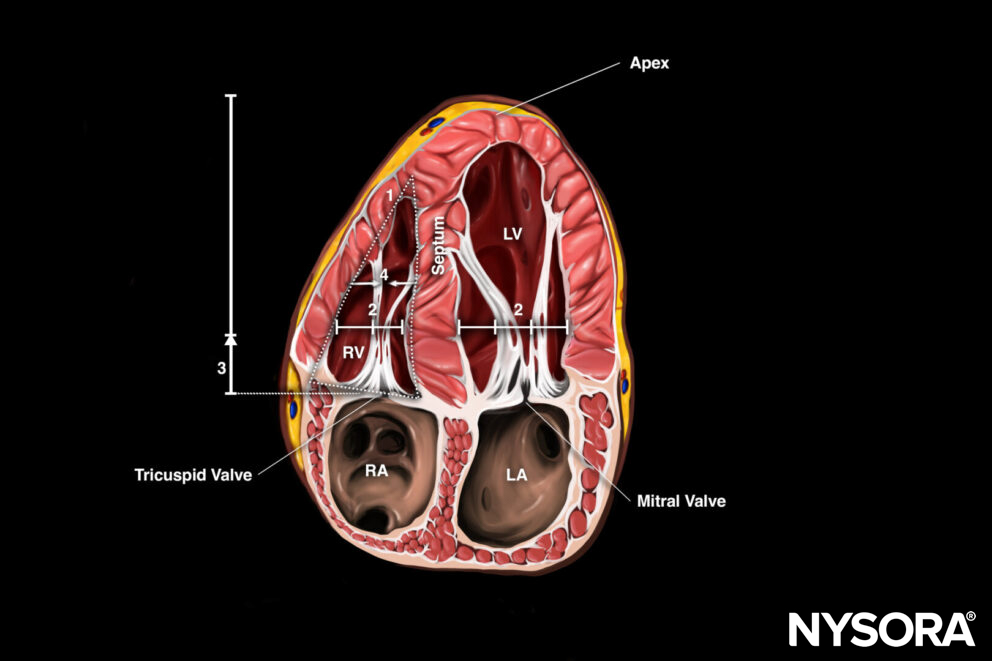
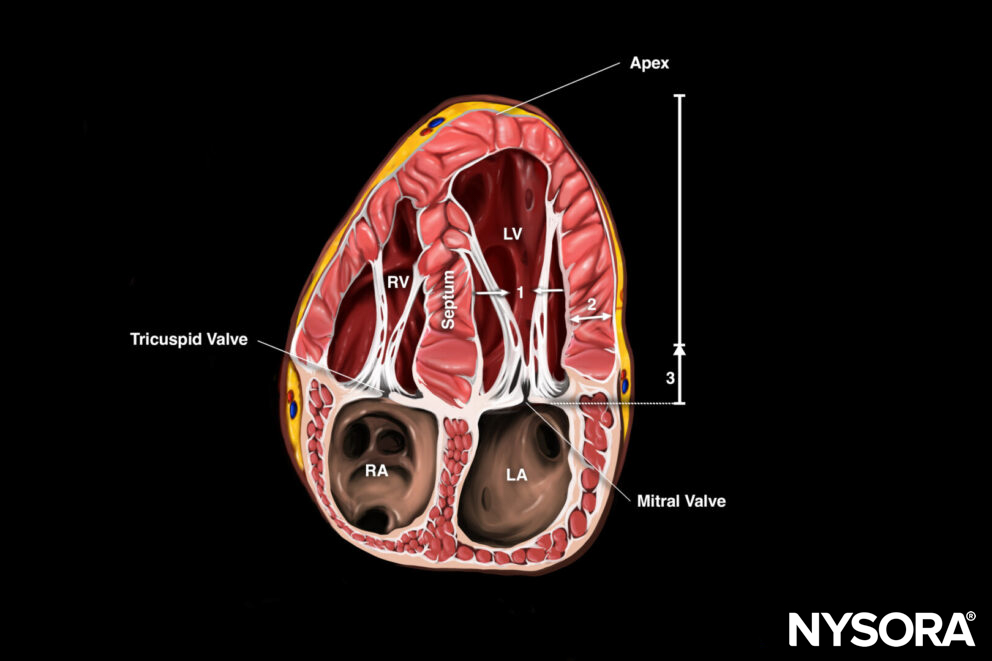
Apical four-chamber view (A4C)
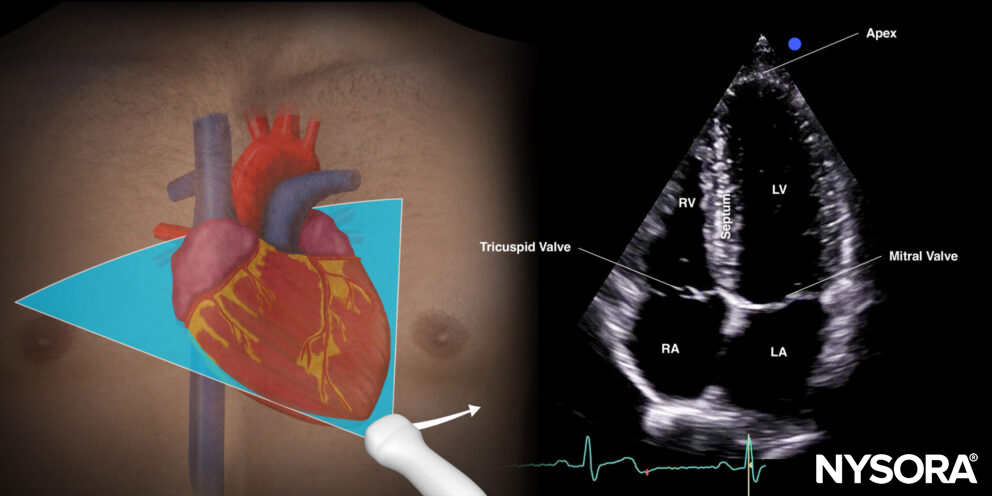
Transducer position and sonoanatomy of the apical four-chamber view.
Assessment
The ‘eyeball method’ estimates the ventricular function (normal vs. reduced) by assessing:
Inward movement of the endocardium during systole (A4C, PLAX, PSAX):
- The left ventricle walls move into the chamber, and the endocardium moves symmetrically toward the center of the left ventricle. Left ventriclular function is good/normal.
- The left ventricular walls move poorly, and the endocardium does not move symmetrically toward the center of the left ventricle. Left ventricular function is likely reduced.
Thickening of the left ventricle wall (myocardium) during systole (A4C, PLAX, PSAX):
- Thickening of the myocardium/left ventricle wall (> 1/3): Left ventricular function is normal.
- No thickening of the myocardium/left ventricle wall (< 1/3): Left ventricular function is likely reduced.
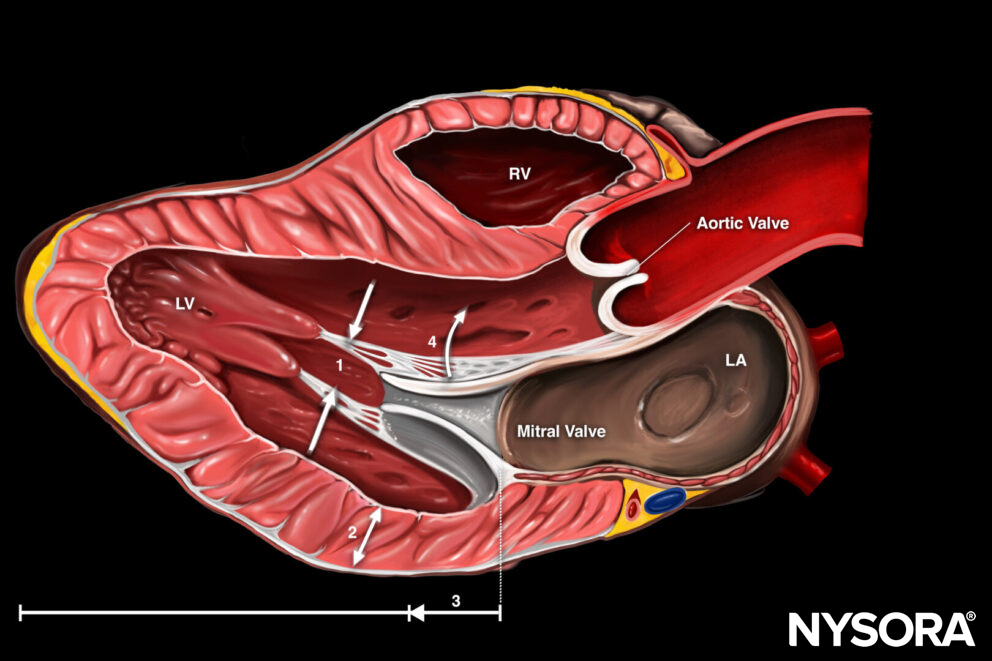
Longitudinal shortening during systole (A4C, PLAX):
- There is a clear difference between the maximal and minimal distance between the base (mitral valve annulus) and the apex of the heart during systole (>1 cm): Left ventricular function is good/normal.
- The difference between the maximal and minimal distance between the base and the apex of the heart during systole is small (<1 cm): Left ventricular function is likely reduced.
Motion of the anterior leaflet of the mitral valve toward the septum (PLAX):
- Approximation of the anterior mitral valve leaflet is good, or the distance between the anterior mitral valve leaflet and the septum is <1 cm: Left ventricular function is good/normal.
- Poor approximation of the anterior mitral valve leaflet or the distance between the mitral valve leaflet and the septum is >1 cm: Left ventricular function is likely reduced.
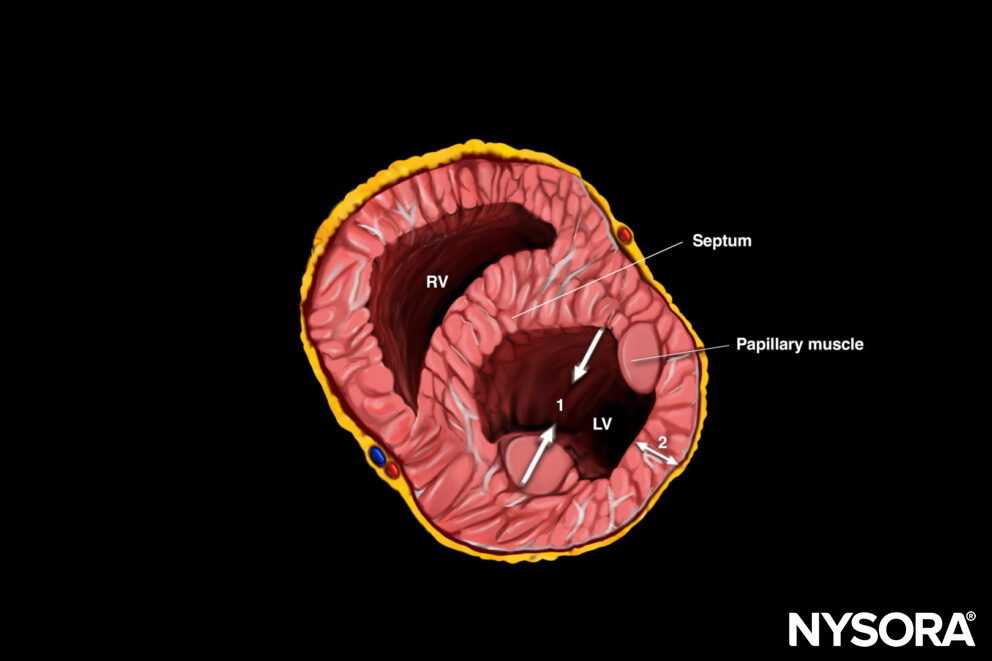
Parasternal short-axis view with 2 motions to be observed for left ventricular function: 1. Inward movement LV walls, 2. Myocardial thickening.
Tip
The motion of the anterior mitral valve leaflet can also be measured using M-mode, and this measurement is called E-Point Septal Separation (EPSS). It measures the distance between the anterior mitral valve leaflet and the septum during maximal excursion of the mitral valve. An EPSS > 1cm correlates with depressed systolic function.
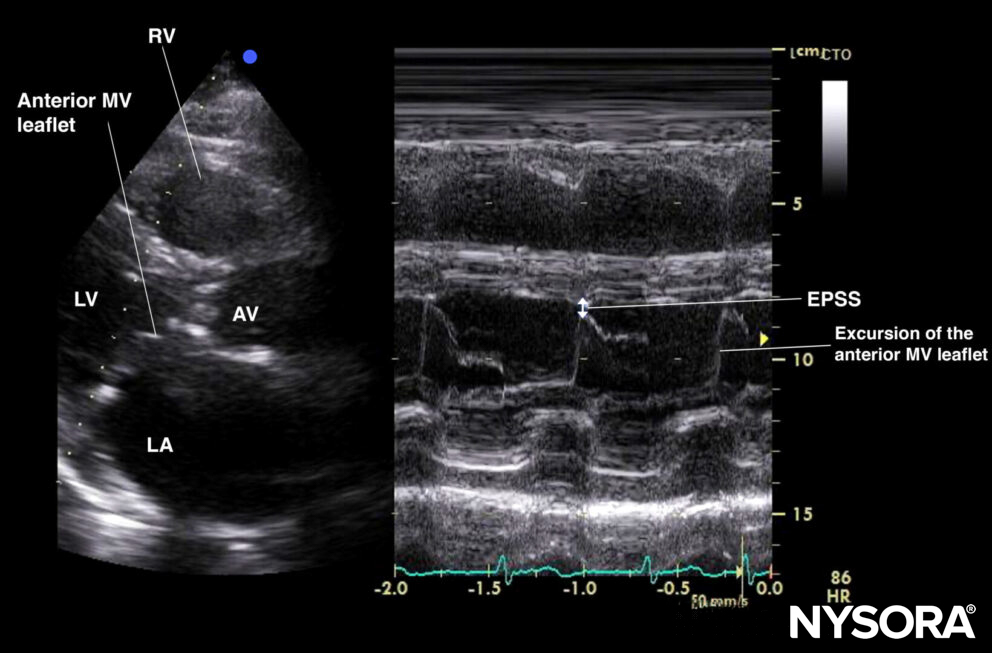
E-point septal separation (EPSS).
- In case of myocardial Infarction, endocardial excursion and myocardial thickening will be affected first. Diminished mitral valve movement is often a late sign.
- In patients with structural heart disease, such as mitral valve stenosis, aortic valve regurgitation, prosthetic valves, or a hypertrophic septum, left ventricular function cannot be reliably estimated by the eyeball method.
- Place a cursor or pointer in the center of the left ventricle to evaluate movements.
Clinical updates
Lebeau et al. (BMC Cardiovascular Disorders, 2023) validated a simplified semi-quantitative wall motion score (WMS) method using only two POCUS views—mid-parasternal short-axis (PSAX-MID) and apical 4-chamber (MID-4CH)—to estimate LVEF by averaging 8 segmental EF values (normal = 60%, hypokinesia = 40%, akinesia = 10%, etc.). In 46 patients (mean LVEF 34 ± 10%), the MID-4CH method showed excellent correlation with the reference 16-segment WMSI-derived LVEF (r² = 0.90), minimal bias (−0.2%), and good precision (±3.3%), and also correlated strongly with Simpson’s biplane EF (r² = 0.92). Emergency physicians achieved similar accuracy (r² = 0.90), supporting this two-view approach as a rapid, reliable LVEF estimation tool for non-cardiologists performing cardiac POCUS.
- Lebeau R, Robert-Halabi M, Pichette M, et al. Left ventricular ejection fraction using a simplified wall motion score based on mid-parasternal short axis and apical four-chamber views for non-cardiologists. BMC Cardiovasc Disord. 2023;23(1):115.