Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
AboutIndications
- Femoral artery cannulation is used for invasive blood pressure monitoring and arterial blood sampling.
- Femoral artery cannulation should be performed when radial artery cannulation is not feasible.
Tip
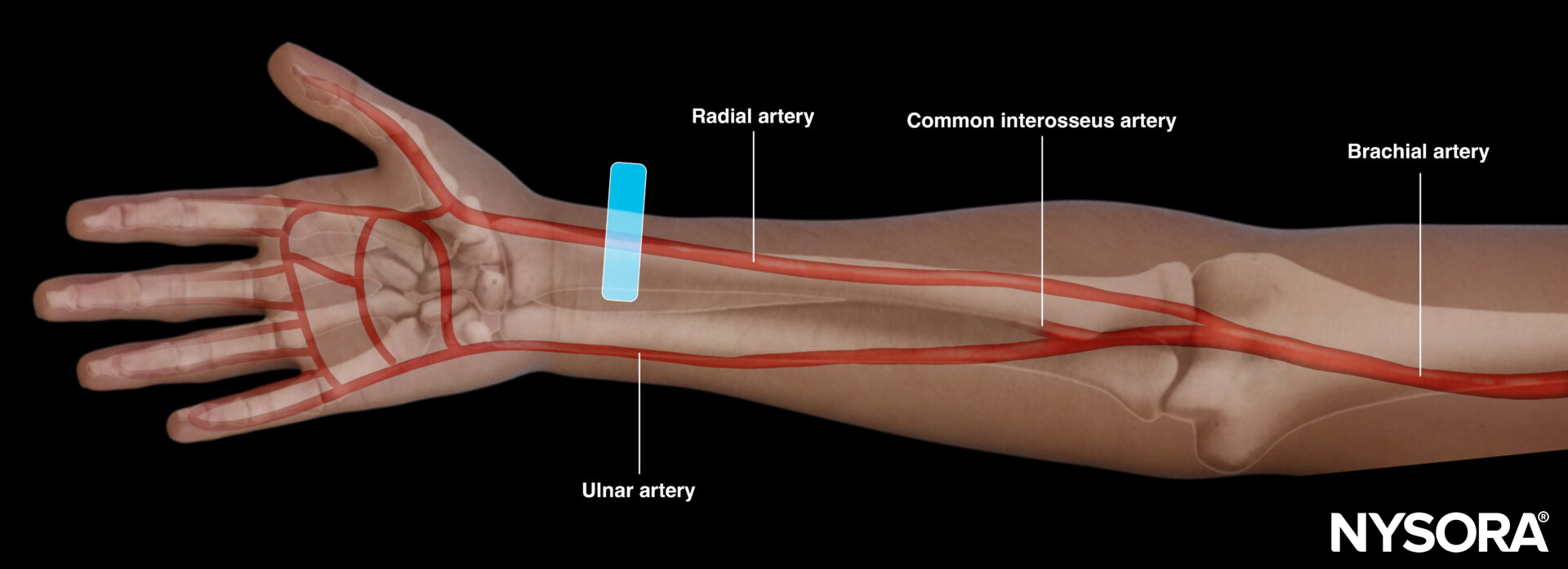
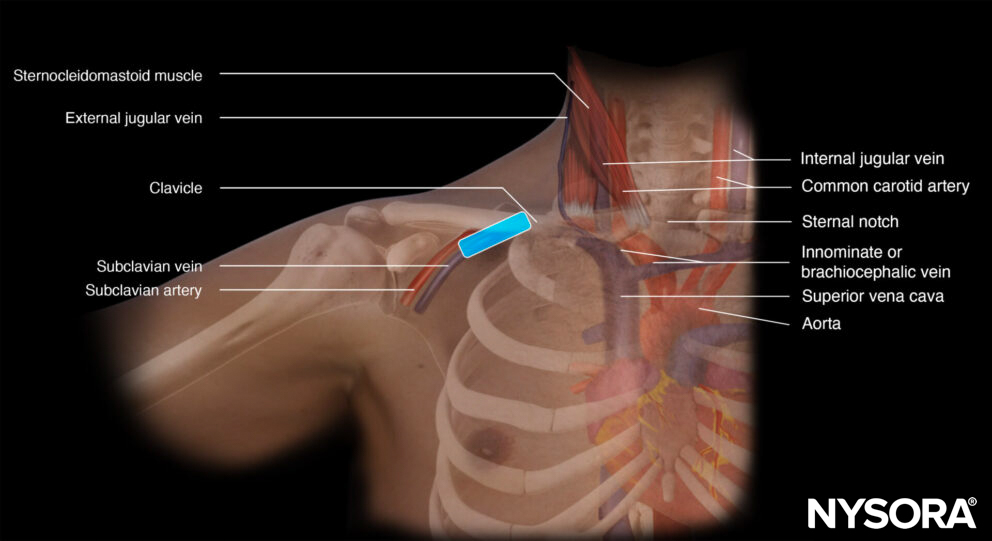
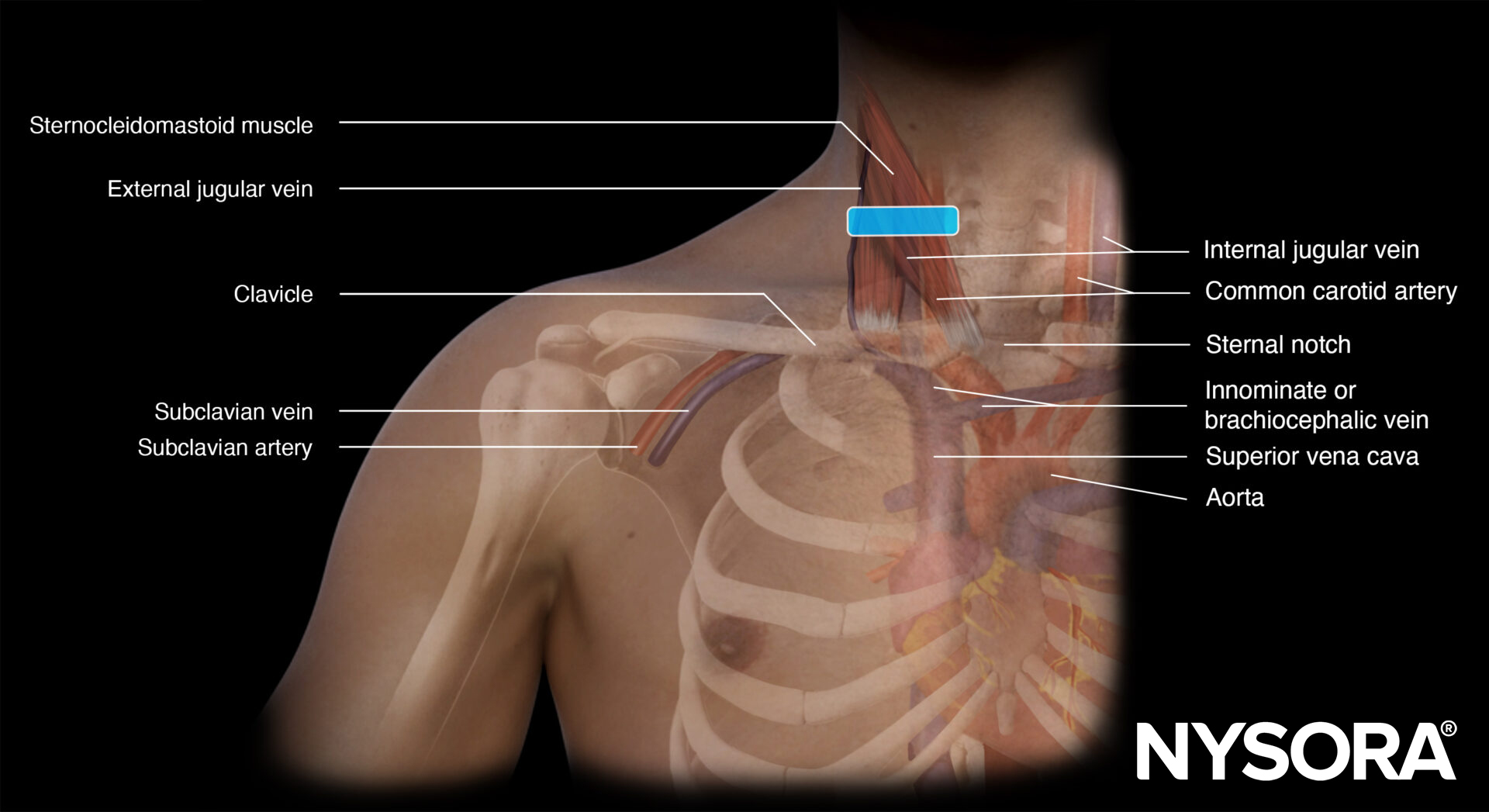
Other cannulation sites (i.e., brachial, ulnar, axillary, dorsalis pedis, tibialis posterior, and temporal artery) should not be considered first-line for insertion due to their higher complication rate.
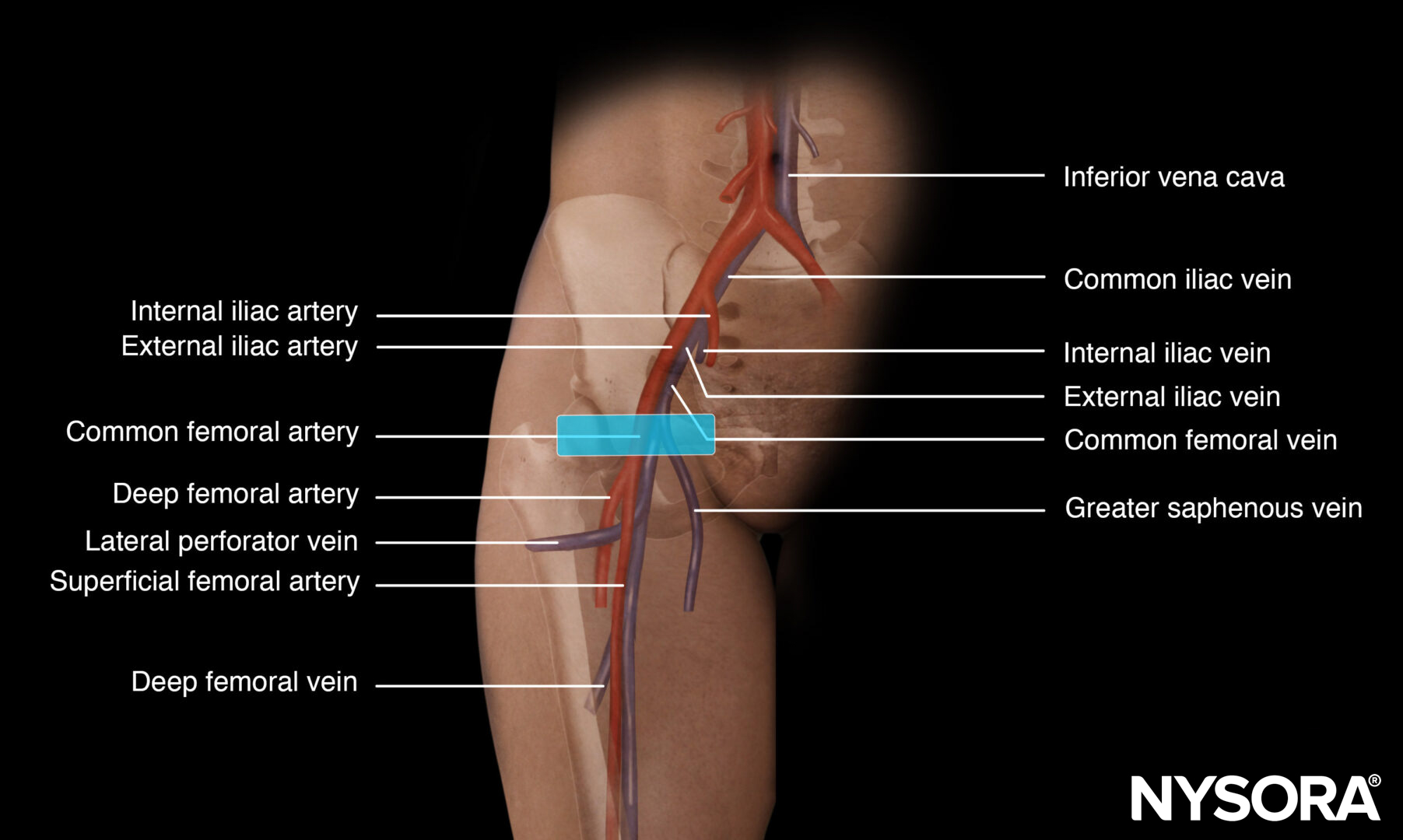
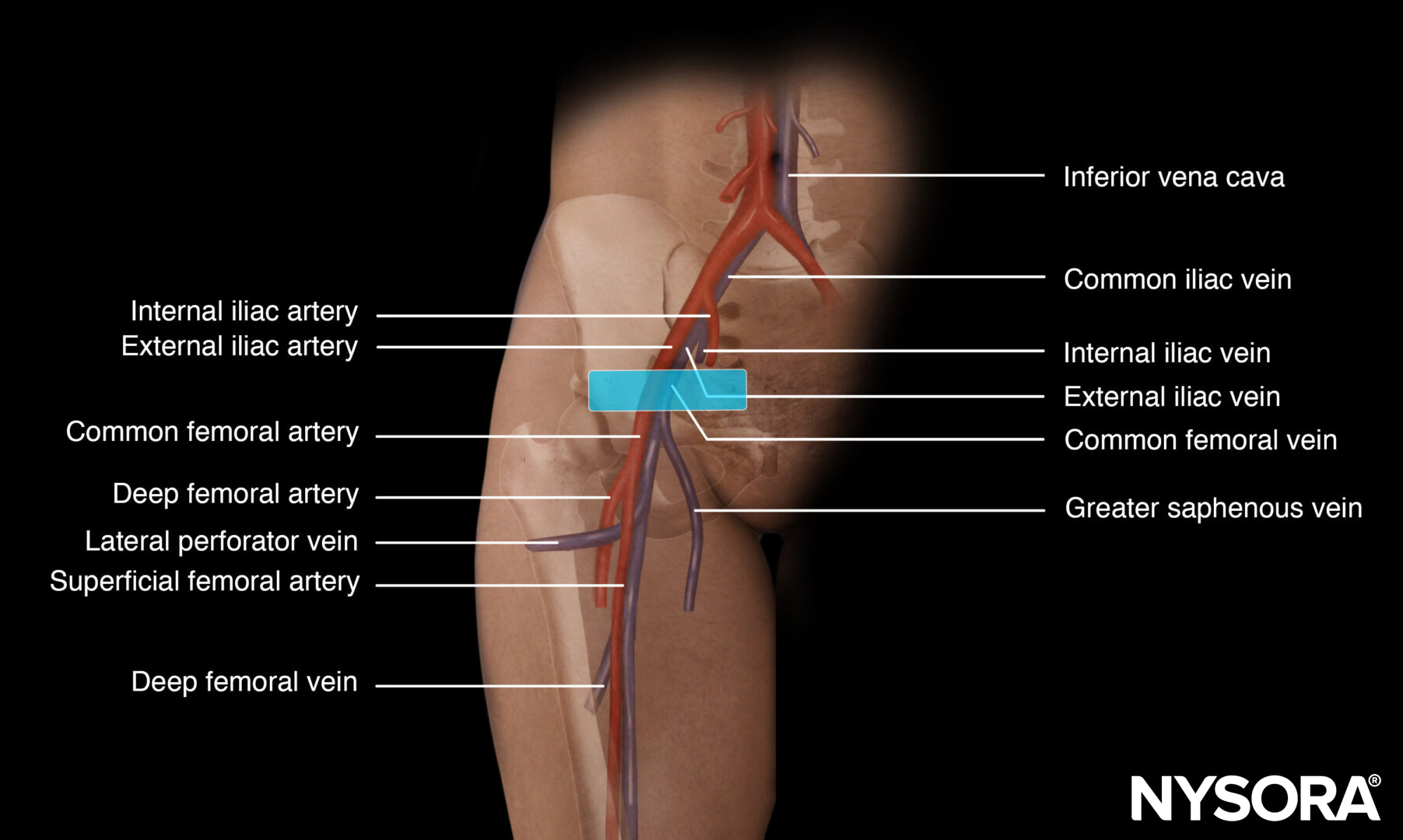
Functional anatomy
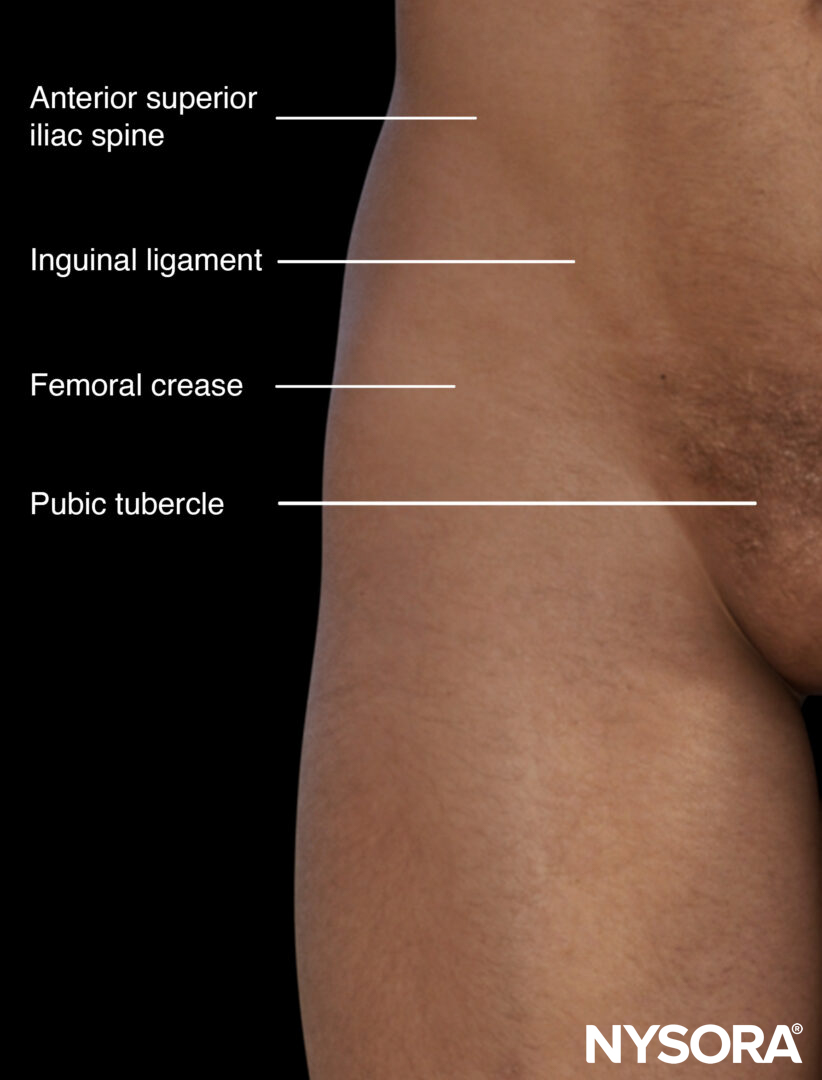
External landmarks of the inguinal area.
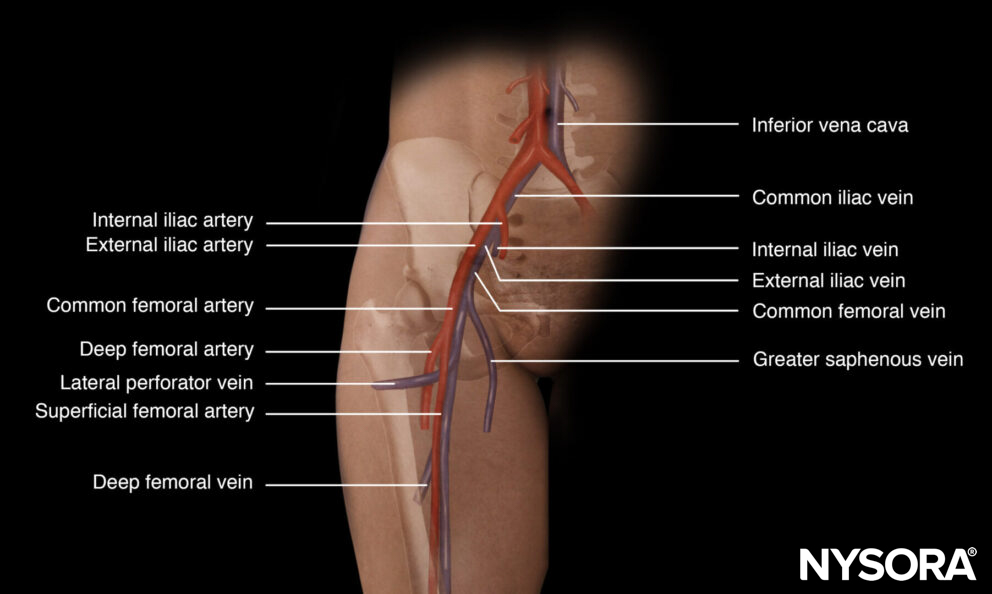
Anatomy of the femoral artery.
Preparation
- Hand hygiene
- Disinfect the area of interest (2% chlorhexidine in 70% isopropyl alcohol)
- Use a sterile drape
- Wear sterile gloves during the procedure
- Use a sleeve or Tegaderm to cover the transducer
- Use sterile gel
- 20G needle with a long cannula
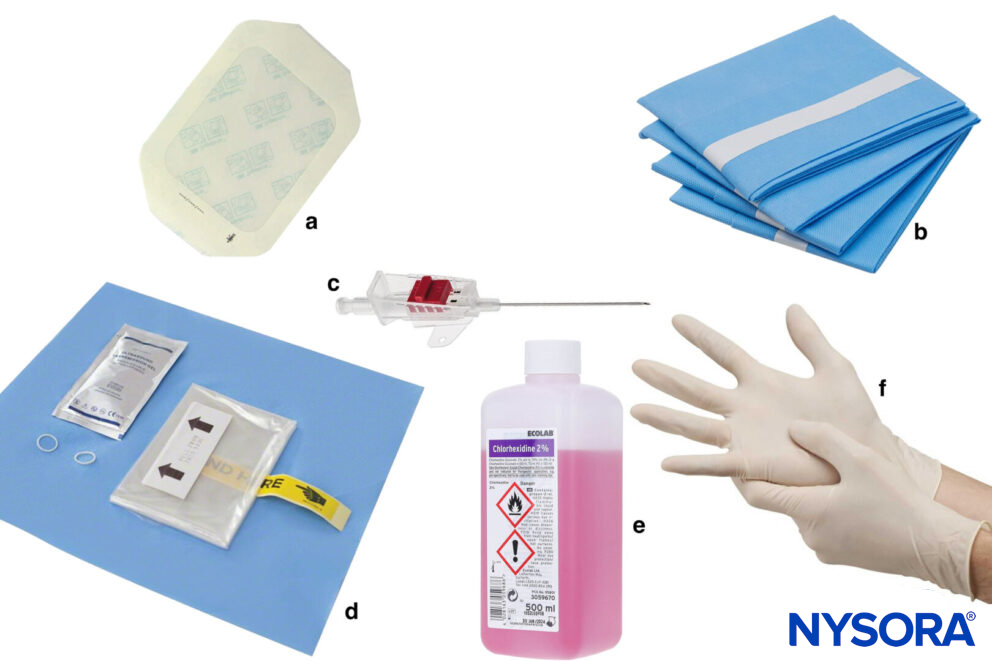
a, Tegaderm; b, Sterile draping; c, Cannula; d, Sterile ultrasound sleeve; e, Antiseptic; f, Sterile gloves.
Patient position
- Femoral artery cannulation is performed in the supine position.
- Expose the extremity of interest.
- Position yourself at a 90-degree angle toward the structure.
- In larger patients, a pillow under the pelvis and slight exorotation of the leg can improve exposure of the inguinal area.
Technique
Position the transducer on the medial third of the line that connects the pubic tubercle with the anterior superior iliac spine or the inguinal ligament. Then scan 1-2 cm distal for the actual puncture.
Transducer position for femoral artery cannulation.
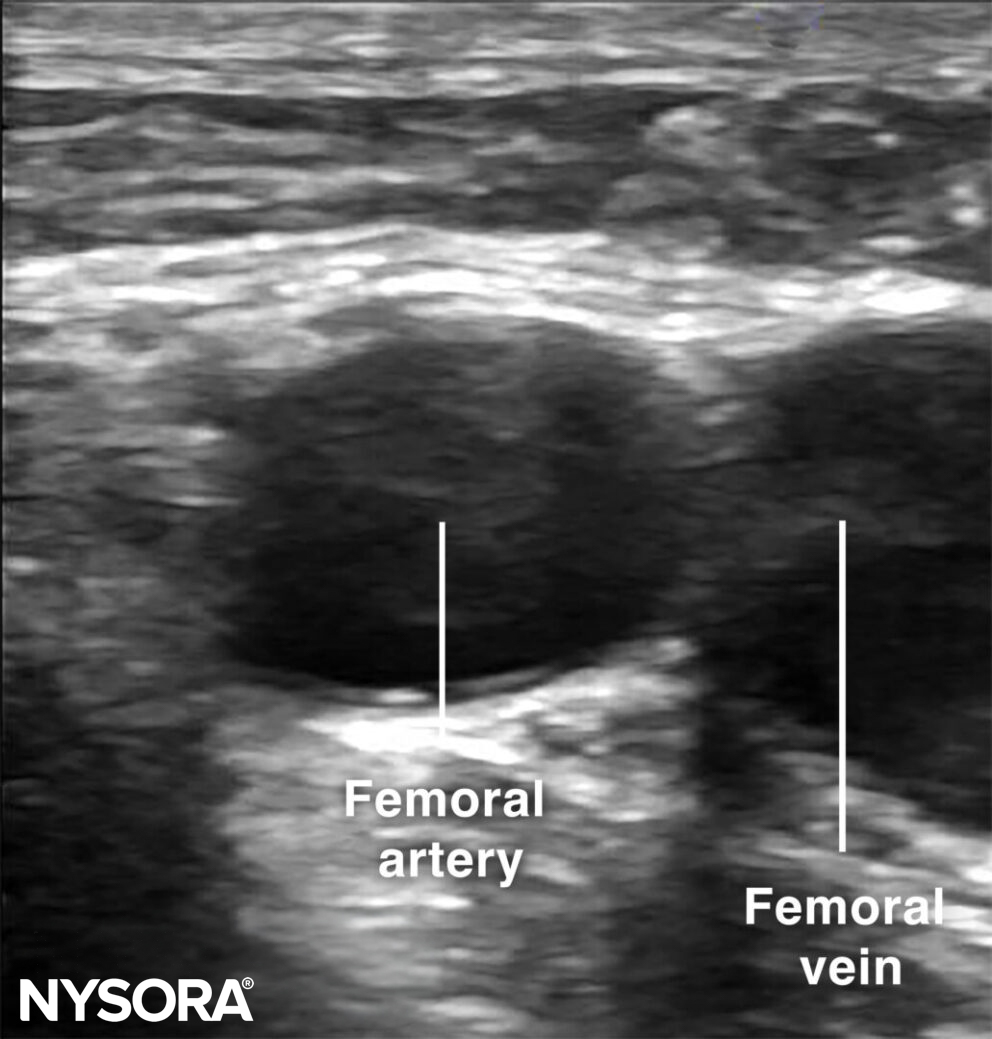
Sonoanatomy for femoral artery cannulation.
The out-of-plane technique is the most commonly used technique for arterial vascular access. Before the actual puncture, scan dynamically to get an idea of the artery’s direction. Use the creep technique to follow the needle tip at all times.
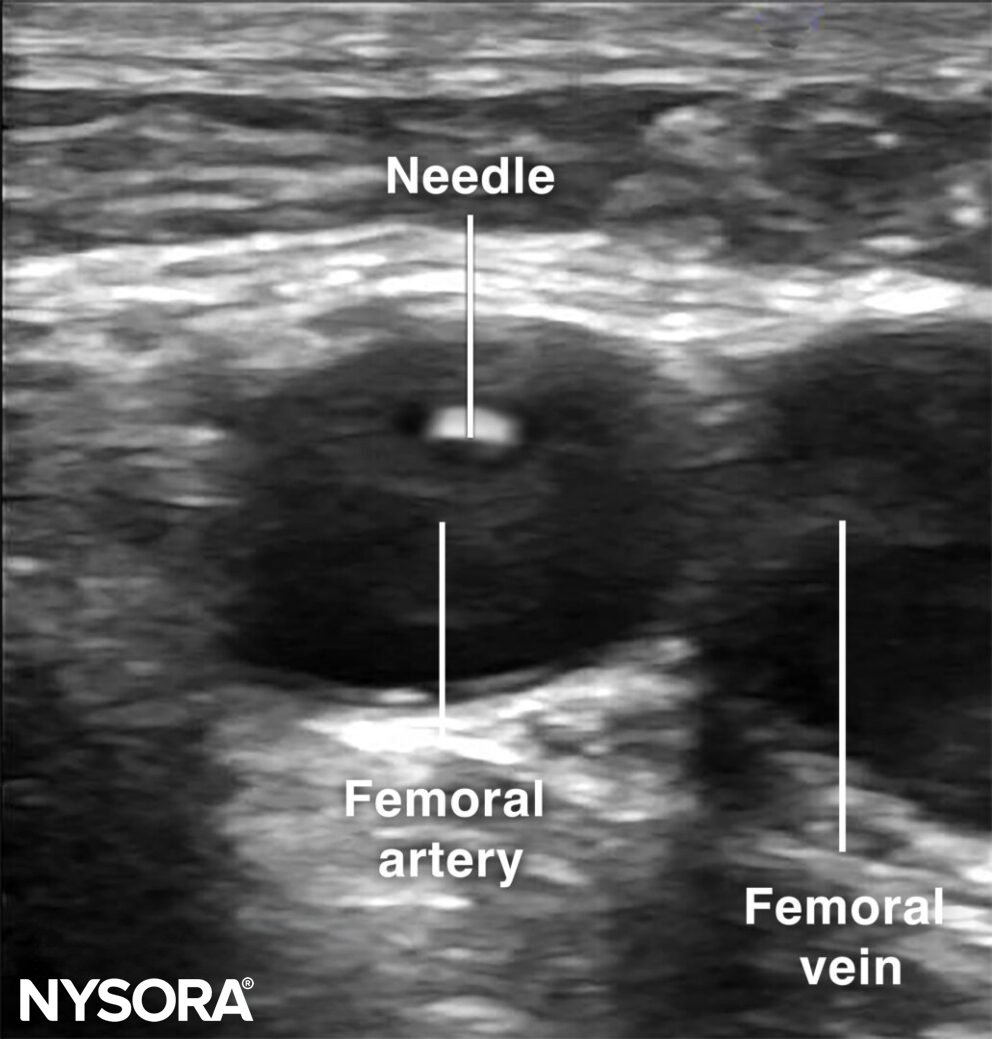
Out-of-plane cannulation of the femoral artery.
Tips
- If two arteries are seen at the level of the femoral artery, it is necessary to scan more proximally.
- Temporary occlusion, hematoma, pseudoaneurysm, nerve injury, ischemia, local infection, and sepsis are the most common complications of arterial cannulation.
Clinical updates
- Bernardi et al. (Catheterization and Cardiovascular Interventions, 2025) describe a standardized six-step ultrasound-guided protocol to achieve a “perfect” common femoral artery (CFA) puncture, defined by anterior-wall-only entry within the CFA, centralized lumen access, puncture above the femoral head, and avoidance of diseased segments, to improve safety and reproducibility. The article integrates real-time longitudinal needle tracking, ultrasound confirmation of guidewire position, and multimodality calibration (CT, fluoroscopy, ultrasound) to reduce the risk of high/low sticks and retroperitoneal bleeding. Citing contemporary RCTs and meta-analyses, the authors highlight higher first-pass success (~82% vs 59%) and lower vascular complications (1.3% vs 3.0%) with ultrasound guidance, supporting routine adoption despite a defined learning curve.
Bernardi FLM, Bernardi GLM, Barbiero JR, et al. A Six-Step Approach for Optimizing Ultrasound-Guided Femoral Artery Access. Catheter Cardiovasc Interv. 2025;106(2):1023-1031.