Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
AboutGoal
Assessment of the function of the right ventricle: normal vs. reduced.
Right ventricular dysfunction can be caused by:
- Decreased contractility
- Right ventricle infarct
- Cardiomyopathy
- Volume overload
- Tricuspid or pulmonic valve regurgitation
- Pressure overload
- Pulmonary embolism
- Left-sided cardiomyopathy or valvular disease
- Pulmonary hypertension (obesity, obstructive sleep apnea syndrome)
- Acute respiratory distress syndrome (hypoxic vasoconstriction)
Views
Parasternal long-axis view (PLAX)

Transducer position and sonoanatomy of the parasternal long-axis view.
Parasternal short-axis view (PSAX)
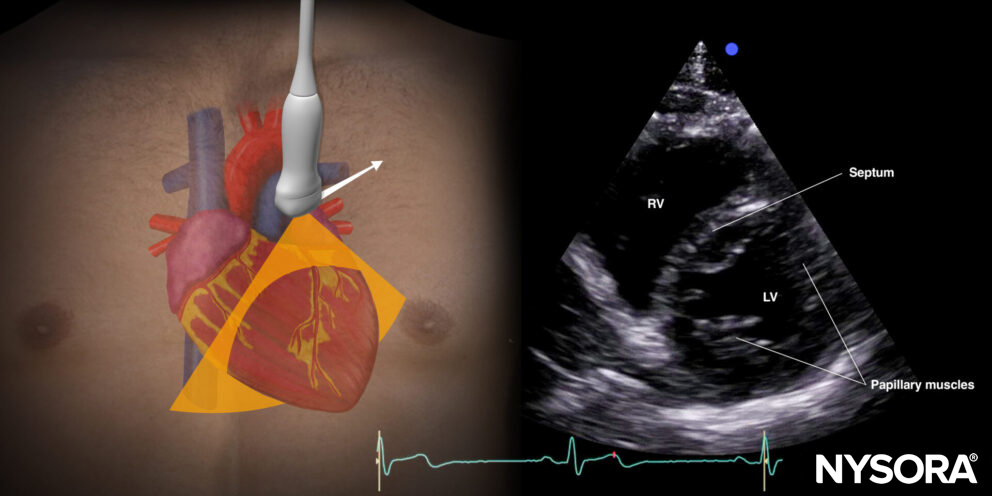
Transducer position and sonoanatomy of the parasternal short-axis view.
Apical four-chamber view (A4C)
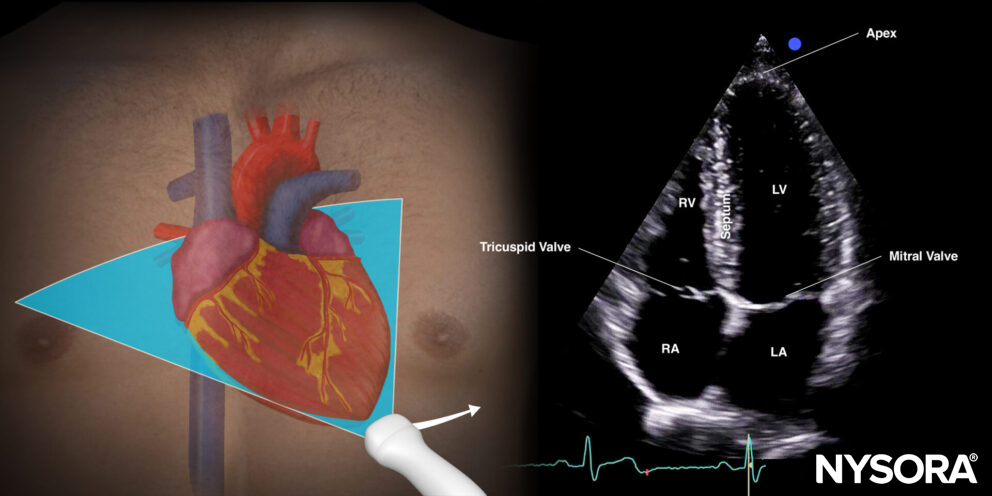
Transducer position and sonoanatomy of the apical four-chamber view.
Assessment
The ‘eyeball method’ estimates the ventricular function (normal vs. reduced) by assessing:
Shape of the right ventricle (PSAX, A4C)
- A crescent or sickle shape in the PSAX view with a rounded septum toward the right ventricle exhibits normal right ventricular function. There is right ventricular dysfunction or pulmonary hypertension when the septum is deviated toward the left ventricle, resulting in a ‘D-shaped’ left ventricle (D-sign).
- A triangular shape in the A4C view, with the annulus of the tricuspid valve as the base and the straight ventricle wall and septum as legs of the triangle, is normal. The LV must also dominate the apex. A convex free wall and septum are typical for right ventricle dysfunction or pulmonary hypertension, as well as a dominant right ventricle.
Size of the right ventricle (PLAX, PSAX, A4C)
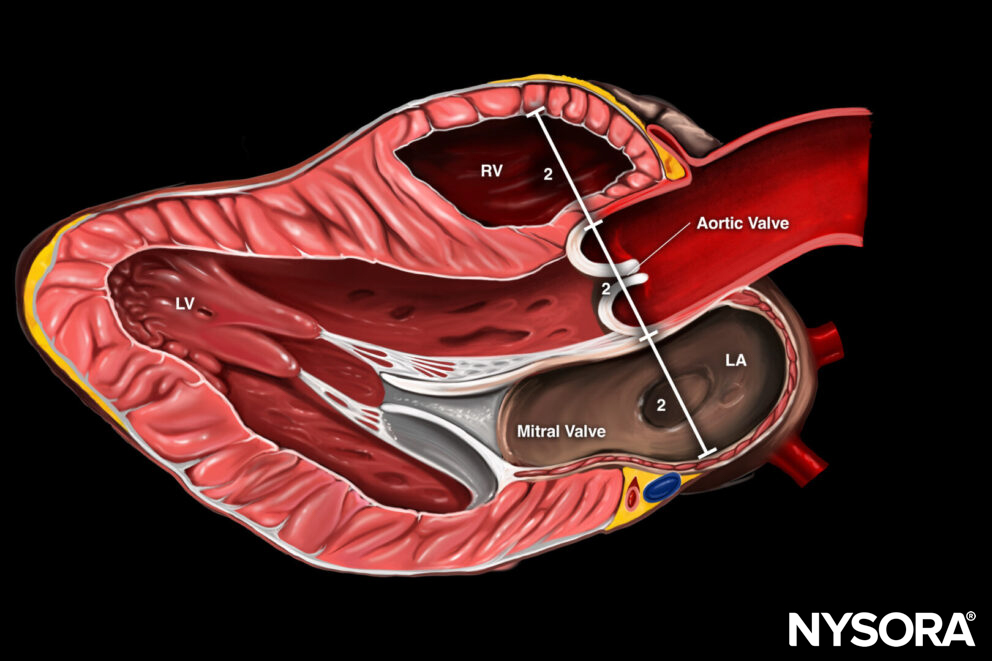
- The rule of thirds is often used for the PLAX view. The diameter of the right ventricle, the annulus of the aorta, and the left atrium should be of similar size.
- Right ventricular size < 2/3 of the left ventricular size indicates normal right ventricular function.
- Right ventricular size > 2/3 of the left ventricular size indicates right ventricular dysfunction or pulmonary hypertension.
Longitudinal shortening of the right ventricle (A4C)
- Assess tricuspid valve annulus movement: best assessed at the level of the right ventricular free wall; can be assessed qualitatively (good/bad) or quantitatively (>16mm: normal; 16mm or less: abnormal).
Inward movement of the free right ventricular wall (PSAX, A4C)
- The contraction of the right ventricle is more peristaltic compared to the left ventricle, but the free wall should move toward the septum.
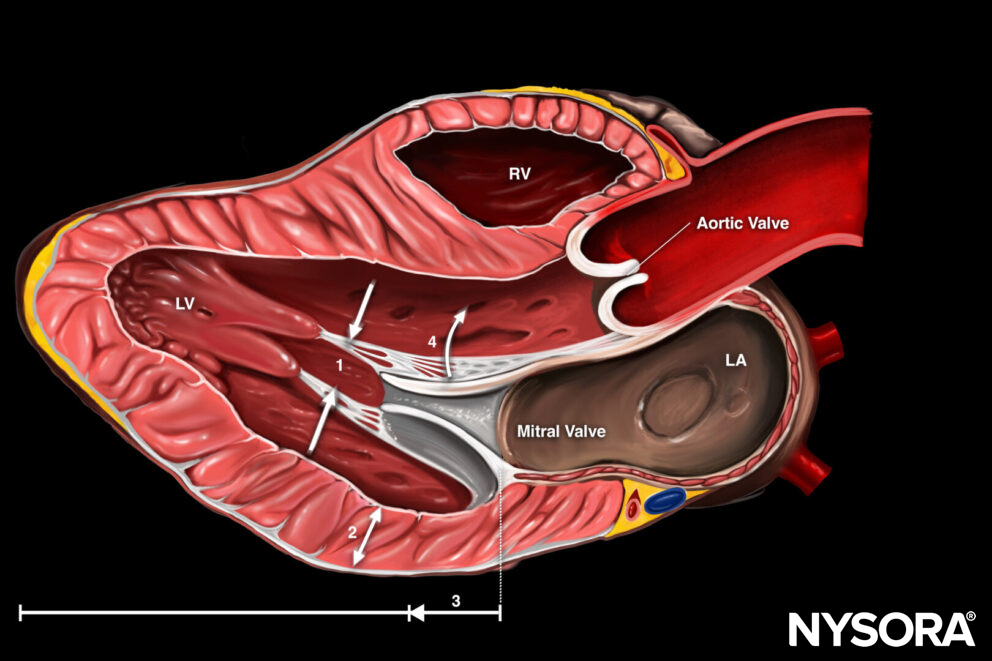
Parasternal long-axis view with 1 assessment for right ventricular function: 2. right ventricular size (rule of thirds).
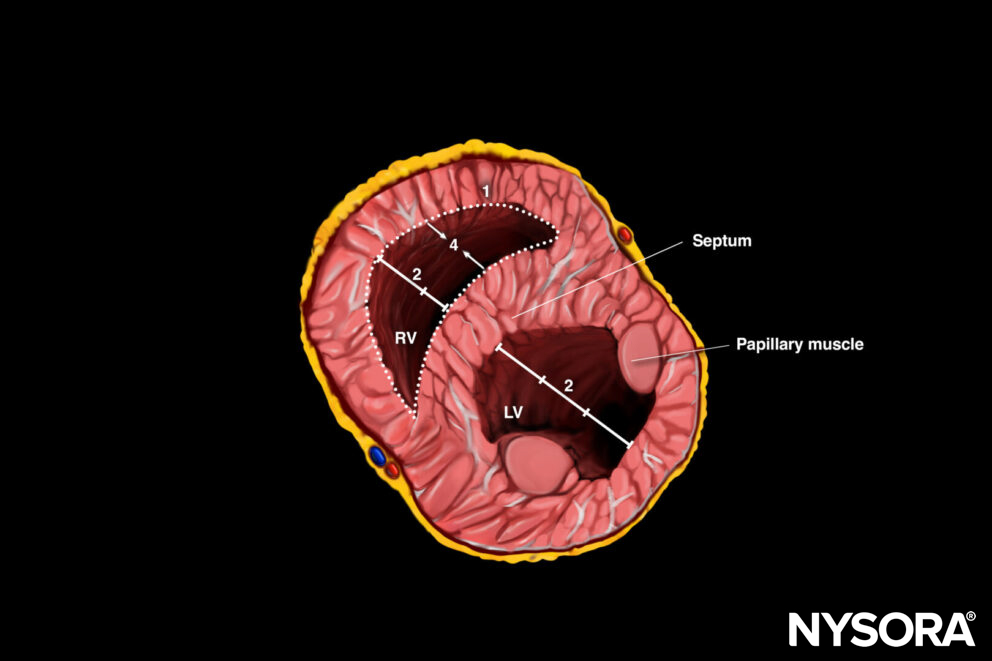
Parasternal short-axis view with 3 assessments for right ventricular function: 1. Shape, 2. Size, 4. Inward motion free RV wall.
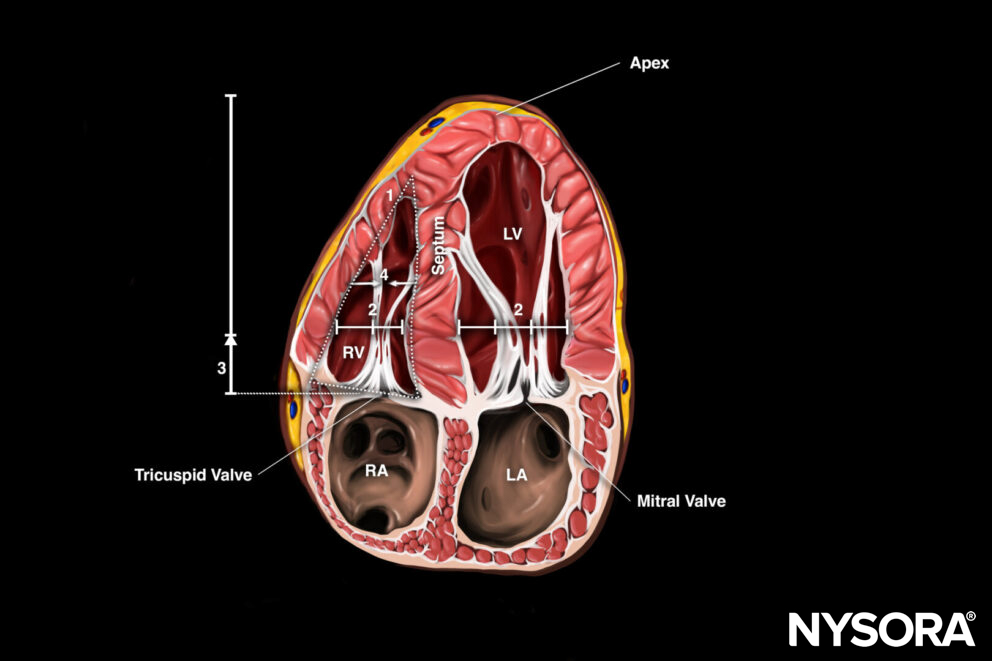
Apical four-chamber view with 4 assessments for right ventricular function: 1. Shape, 2. Size, 3. Longitudinal shortening, 4. Inward motion free RV wall.
Tips
- Longitudinal shortening is also called TAPSE (Tricuspid Annular Plane Systolic Excursion) and can be measured by using the M-mode through the tricuspid annulus at the level of the free wall: a normal right ventricular function will result in a difference of > 16 mm when comparing minimal to maximum excursion of the annulus.

Tricuspid Annular Plane Systolic Excursion (TAPSE).
- The right ventricle anatomy is complex.
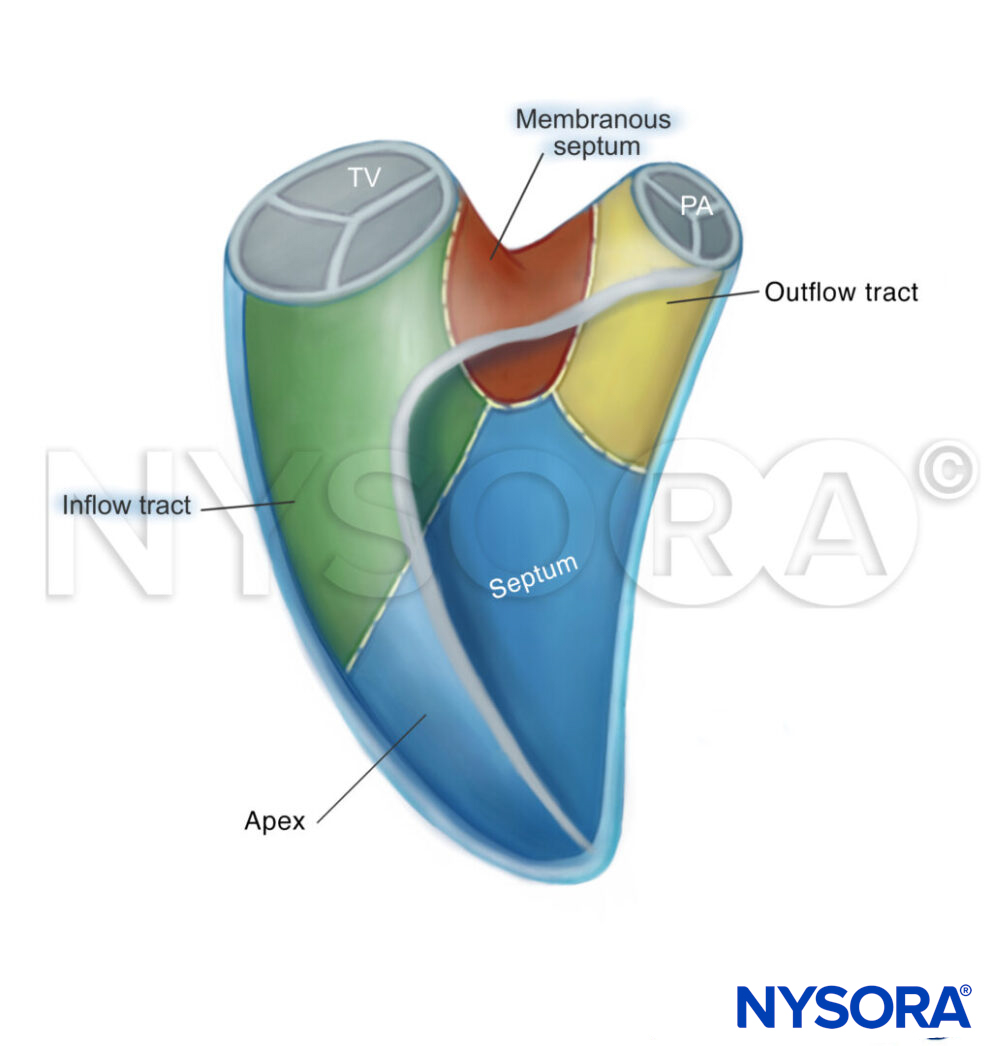
Anatomy and shape of the right ventricle: inflow tract – apex – membranous septum – outflow tract.
- The thickness of the free right ventricular wall is another parameter used to assess right ventricular function. It is, however, not always visible and, therefore not included into our standard assessment.
- Free wall < 5mm: Normal
- Free wall > 5mm: Chronic or acute on chronic heart failure
- Right ventricular assessment is essential in the point-of-care stratification of pulmonary embolism. If the right ventricle appears normal, a life-threatening pulmonary embolism is unlikely.
- The subcostal views can be used as a backup to the apical or parasternal views, e.g., in ventilated or COPD patients.
- The right ventricle will dilate acutely under abnormal conditions, as it is not accustomed to pumping against high afterload. This will result in changes in the septal kinetics or D-shaping of the left ventricle.
- Right ventricle enlargement may result in McConnell’s sign: Hypokinesis or akinesis of the right ventricle free wall with hyperdynamic right ventricle apical wall movements.
- Ventricular interdependence is a term that is used to stress that the function of one ventricle may be influenced by the other one. The increase in volume of one ventricle will result in a decrease in volume of the left ventricle.
Clinical updates
Prakash et al. (International Journal of Emergency Medicine, 2025) conducted a prospective observational study of 172 ED patients undergoing drug-assisted intubation and found that 41.2% developed post-intubation hypotension (PIh), with significantly lower pre-intubation TAPSE values in those who became hypotensive (17.66 ± 2.45 mm vs. 18.54 ± 2.15 mm, p=0.014). Multivariable analysis identified TAPSE as an independent predictor of PIh (OR 0.81, 95% CI 0.69–0.95, p=0.009), and ROC analysis showed moderate discrimination (AUC 0.584), with a cutoff of 17.6 mm yielding 85.1% sensitivity but low specificity (29.6%). These findings support rapid pre-intubation RV assessment with TAPSE as a practical POCUS-based risk stratification tool for identifying patients at high risk of peri-intubation hemodynamic collapse
- Prakash P, S N, Balakrishnan JM, Alli SD, S RG, Naik SR. Right ventricular dysfunction: a key predictor of post-intubation hypotension in the emergency department. Int J Emerg Med. 2025;18(1):183.