Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About



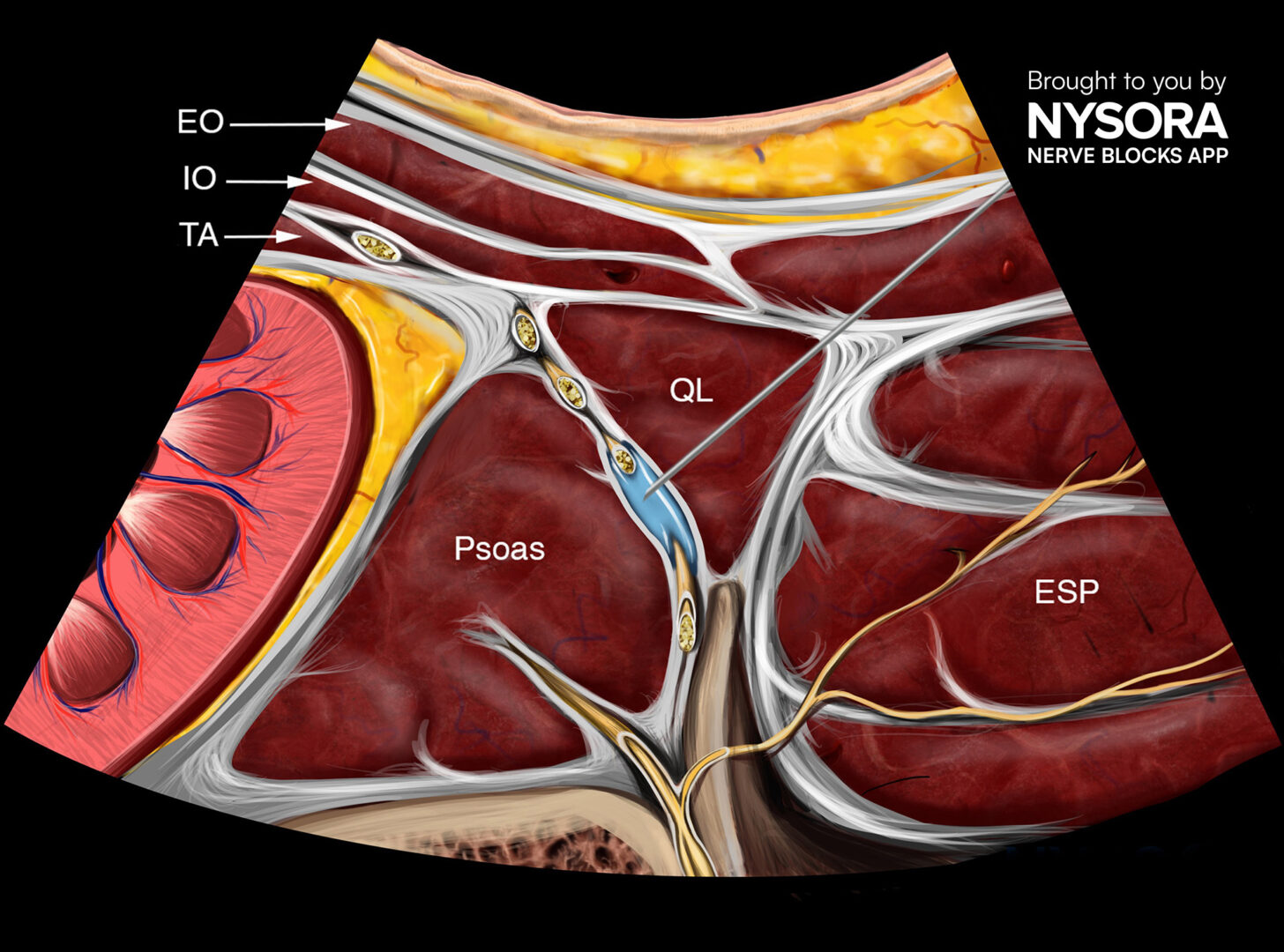
Early mobilization, effective pain management, and optimized patient recovery are essential components of enhanced recovery after surgery (ERAS) protocols. To support these goals, the anterior quadratus lumborum (QL) block has emerged as a widely used regional anesthesia technique, particularly valued for its dual somatic and visceral analgesic effects in abdominal and retroperitoneal surgeries. This block is typically administered at the L3–L4 vertebral level, where local anesthetic is injected into the fascial plane between the quadratus lumborum and psoas major muscles, posterior to the transversalis fascia.
Despite its clinical utility, the anatomical proximity of the anterior QL block to the lumbar plexus—especially the femoral nerve—has raised concerns about potential motor weakness. In particular, the inadvertent spread of local anesthetic to motor branches can result in quadriceps muscle weakness or even temporary paralysis, potentially hindering postoperative ambulation and delaying recovery.
In clinical practice, anecdotal reports have not indicated significant lower limb weakness following this block. Nonetheless, until now, there had been no rigorous, controlled evaluation of its impact on quadriceps motor function in living subjects.
To address this gap, a new randomized, triple-blinded, non-inferiority trial published in Regional Anesthesia & Pain Medicine sought to systematically assess whether the anterior QL block impairs quadriceps strength. The findings could play a pivotal role in determining the safety of this block in fast-track surgical recovery protocols.
Study objective and methods
The primary aim of this study was to evaluate whether a unilateral anterior QL block results in quadriceps muscle weakness, as measured by maximal voluntary isometric contraction (MVIC), when compared with a placebo. Secondary outcomes included functional mobility assessments and dermatomal sensory mapping.
Study design
- Population: 20 healthy adult volunteers (ASA physical status I–II).
- Design: Randomized, controlled, triple-blinded, non-inferiority trial.
- Location: Zealand University Hospital, Roskilde, Denmark.
- Intervention: Each participant received an anterior QL block with 30 mL ropivacaine 0.75% on one side and 30 mL saline (placebo) on the other side.
- Blinding: Participants, clinicians, and outcome assessors were all blinded to allocation.
- Assessment window: 60 minutes post-block administration.
Outcome measures
-
- Primary: Change in quadriceps MVIC (in Newtons).
- Secondary:
-
- Timed-Up and Go (TUG) test.
- 6-meter single-leg timed hop test.
- Mean arterial pressure (MAP).
- Dermatome sensory mapping using cold and pinprick stimuli.
- Safety: Monitoring for adverse events (AEs) and serious adverse events (SAEs).
Key findings
- No clinically meaningful motor block: The difference in MVIC between active and placebo sides was 15.88 N (95% CI: −12.19 to 43.94), falling within the non-inferiority margin of −25 N (p<0.003). This confirms that the anterior QL block did not produce clinically significant quadriceps weakness.
- Secondary outcomes: TUG test improved post-block (−0.23 s, p = 0.005), likely due to a learning effect rather than a physiological change. MAP increased slightly by 4.25 mm Hg (p = 0.04), but this was not clinically relevant. The hop test showed no significant difference between sides.
- Sensory distribution: Dermatomal testing revealed sensory changes mainly in the Th10–L1 range, corresponding to lower abdominal areas. No participants had sensory loss below L3, suggesting the femoral nerve remained unaffected.
- Safety profile: Five minor AEs were recorded (e.g., transient nausea, vasovagal reactions), all resolving without intervention. No SAEs were observed. All participants were discharged 2 hours post-block with no lingering effects.
Conclusion
This trial provides the first controlled evidence that an anterior QL block performed at the L3/L4 level does not impair quadriceps muscle strength in healthy volunteers. This finding supports its safe inclusion in ERAS protocols, particularly where rapid postoperative mobilization is critical.
Notably, the block offered sensory coverage primarily in the lower abdominal region without extending to motor branches of the lumbar plexus. This aligns with anatomical studies showing minimal dye spread to the femoral nerve when the block is correctly placed.
Future research
While these results are promising, the study population consisted of healthy, young volunteers. Further research is needed to assess the block’s safety and efficacy in actual surgical patients, particularly those with:
- Higher BMI or comorbidities.
- Undergoing major abdominal or pelvic surgeries.
- Receiving bilateral or repeated regional blocks.
Key directions for future investigation:
- Clinical outcome studies: Testing in surgical settings, such as laparoscopic hysterectomy, nephrectomy, or colectomy.
- Anatomical variability: Exploring how lumbar plexus variants affect block spread.
- Comparison trials: Evaluating anterior QL block versus other truncal or plexus blocks for both analgesia and motor preservation.
Clinical implications
For procedures requiring effective pain relief without motor impairment—such as laparoscopic surgery, urology, or day-case abdominal procedures—the anterior QL block offers a viable, motor-sparing alternative. Its compatibility with ERAS goals makes it a strong candidate for broader adoption in perioperative pain protocols.
By confirming the absence of quadriceps weakness, this study alleviates longstanding concerns and strengthens the case for anterior QL block in modern regional anesthesia practice.
Clinical pearls
- QL block at L3–L4: No clinically significant reduction in quadriceps MVIC.
- Sensory coverage: T10–L1; no spread below L3.
- No motor impairment → preserves ambulation, aligns with ERAS.
- Safe profile: Only minor AEs, no SAEs observed.
Practical tip: For laparoscopic or day-case abdominal surgery, the anterior QL block provides analgesia without motor risk—ideal for fast-track recovery.
For more detailed information, refer to the full article in RAPM.
Tanggaard K. et al. No quadriceps muscle weakness following anterior quadratus lumborum block compared with placebo: a randomized, non-inferiority, blinded, volunteer trial. Reg Anesth Pain Med. 2025;50:568-574.
Want to master the anterior QL block? Subscribe to the NYSORA Nerve Blocks App for step-by-step technique guides, sonoanatomy, and expert tips.
Would you consider incorporating the anterior quadratus lumborum block into your ERAS protocols—and why or why not?