Learning objectives
- Discuss the perioperative management of patients with hypotension
- Describe the management of hypotension
Definition and mechanism
- Frequently used definitions are:
- A systolic arterial pressure (SAP) < 80 mmHg
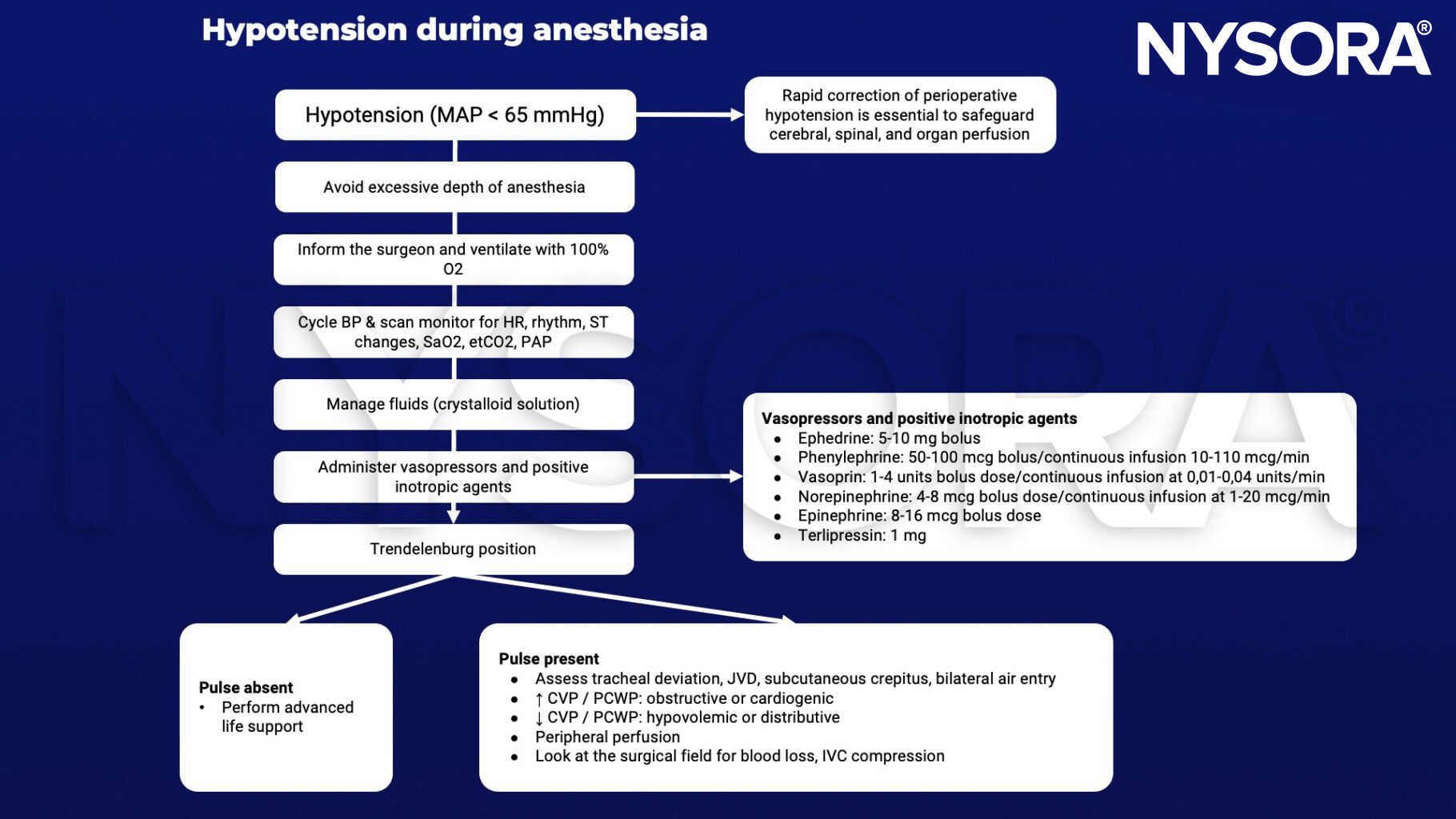
- A MAP < 65 mmHg
- A decrease of 10-60% in baseline MAP or SAP
- Caused by excessive vasodilation or insufficient constriction of arterioles
- Due to decreased sympathetic nervous system output or increased parasympathetic activity
Signs and symptoms
- Cold, clammy skin
- Decrease in skin coloration (pallor)
- Rapid, shallow breathing
- Weak and rapid pulse
Causes
- Vasodilation
- Intravascular hypovolemia
- Anaphylaxis
- Sepsis/SIRS
- Anesthetic agent overdose or swap
- Low cardiac output
- High intrathoracic pressure
- Impairment of sympathetic nervous system
- Compromised baroreflex regulation
Risk factors
- Older age
- High ASA class
- Male lex
- Lower pre-induction SAP
- General anesthesia with propofol
- Combination of general and regional anesthesia
- Duration of surgery
- Emergency surgery
- Antihypertensive medications (ACE inhibitors, A2 receptor antagonists, beta blockers or alpha-2 agonists)
Management
Postoperative complications
- Myocardial injury
- Myocardial infarction
- Cardiogenic shock
- Acute kidney injury
- Delirium
- Stroke
- Death
Suggested reading
- Weinberg L, Li SY, Louis M, et al. Reported definitions of intraoperative hypotension in adults undergoing non-cardiac surgery under general anaesthesia: a review. BMC Anesthesiol. 2022;22(1):69.
- Guarracino, F., Bertini, P. Perioperative hypotension: causes and remedies. J Anesth Analg Crit Care 2, 17 (2022).
- Kouz K, Hoppe P, Briesenick L, Saugel B. Intraoperative hypotension: Pathophysiology, clinical relevance, and therapeutic approaches. Indian J Anaesth. 2020;64(2):90-96.
- Lonjaret L, Lairez O, Minville V, Geeraerts T. Optimal perioperative management of arterial blood pressure. Integr Blood Press Control. 2014;7:49-59.
Clinical updates
Ripollés-Melchor et al. (Anesthesiology, 2025) report in a multicenter randomized trial of 917 high-risk abdominal surgery patients that Hypotension Prediction Index (HPI)–guided intraoperative management did not reduce moderate-to-severe postoperative AKI compared with standard care, nor did it improve overall complications, mortality, or length of stay. Although HPI accurately predicted impending hypotension and prompted more frequent vasopressor use, this proactive strategy did not translate into improved renal outcomes, underscoring that prediction of hypotension alone is insufficient without optimized, individualized hemodynamic interventions.
Rössler et al. (Anesthesiology, 2025) analyzed 38,940 noncardiac surgeries and found that intraoperative hypotension, defined as MAP < 65 mmHg, was not associated with postoperative delirium, challenging the assumption that this threshold independently drives adverse neurologic outcomes. While higher intraoperative average MAP showed only a weak protective effect, postoperative blood pressure demonstrated a U-shaped association with delirium risk, with both lower and higher MAP and increased postoperative BP variability linked to a higher incidence. These findings suggest that postoperative hemodynamic stability and avoidance of excessive BP variability may be more clinically relevant than strict intraoperative MAP thresholds alone in managing perioperative hypotension risk.
Mukkamala et al. (A&A, 2025) critically review current machine-learning approaches to predicting intraoperative hypotension (IOH), highlighting that while tools such as the Hypotension Prediction Index (HPI) can forecast MAP < 65 mmHg up to 15 minutes in advance, real-world performance is modest, with positive predictive values around 30% and accuracy comparable to simple MAP threshold monitoring. Importantly, although some studies show reduced hypotension exposure with prediction-guided management, there is no consistent evidence of improved organ outcomes, and high false-positive rates may lead to unnecessary fluid and vasopressor use. The authors advocate redefining hypotension using cumulative MAP area-under-the-curve metrics and individualized thresholds to improve both predictive precision and clinical utility in managing intraoperative hypotension.
- Read more about this study HERE.
Lee et al. (A&A, 2025) conducted a systematic review of 48 randomized trials evaluating strategies to prevent intraoperative hypotension (IOH) during major noncardiac surgery and found that while multiple interventions reduce IOH exposure, consistent improvements in hard clinical outcomes remain unproven. Protocolized hemodynamic management, individualized MAP targets, continuous monitoring, preoperative withholding of ACE inhibitors/ARBs, pre-induction fluid optimization, and norepinephrine use all reduced hypotensive episodes, yet few strategies demonstrated clear reductions in mortality, myocardial infarction, or stroke. These findings emphasize that although IOH can be mitigated through multimodal and technology-assisted approaches, translating improved blood pressure control into measurable outcome benefits remains a critical research priority.
- Read more about this study HERE.
Van Herreweghe et al. (European Journal of Anaesthesiology and Intensive Care, 2025) conducted a systematic review of 10 randomized trials comparing isobaric versus hyperbaric spinal bupivacaine in non-obstetric surgery and found a trend toward higher hypotension incidence with hyperbaric formulations, likely due to greater cephalad spread and more extensive sympathetic blockade, though no statistically significant overall difference was demonstrated. Hyperbaric solutions were more frequently associated with higher sensory levels, particularly when administered in the sitting position, which may increase hemodynamic instability. These findings highlight that baricity, dosing, and patient positioning influence spinal anesthesia–induced hypotension, underscoring the need for individualized dosing and standardized definitions of hypotension in clinical practice.
- Read more about this study HERE.