Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Describe ankylosing spondylitis
- Recognize the symptoms and signs of ankylosing spondylitis
- Anesthetic management of a patient with ankylosing spondylitis
Definition and mechanisms
- Ankylosing spondylitis (AS), autoimmune seronegative spondyloarthropathy, is a painful chronic inflammatory arthritis characterized by exacerbations (flares) and quiescent periods
- AS primarily affects the spine and sacroiliac joints, eventually causing fusion and rigidity of the spine → bamboo spine
- Joint mobility in the affected areas worsens over time
- The areas most commonly affected are
- Sacroiliac joints
- Vertebrae in the lower back
- Places where tendons and ligaments attach to bones, mainly in the spine
- Cartilage between the breastbone and the ribs (sternum)
- Hip and shoulder joints
- Linked to HLA-B27 gene
Signs and symptoms
Symptoms might worsen (flares), improve, or stop at irregular intervals
- Chronic dull pain in the lower back or gluteal region combined with stiffness of the lower back, especially in the morning and after periods of inactivity
- Hip pain
- Joint pain
- Neck pain
- Fatigue
- Difficulty breathing
- Loss of appetite and unexplained weight loss
- Abdominal pain and diarrhea
- Skin rash
- Vision problems
Complications
- Spinal compression fractures
- Atlanto-axial subluxation possible (21% of AS patients)
- Eye inflammation (iritis or uveitis) and sensitivity to light (photophobia)
- Fused vertebrae (ankylosis)
- Kyphosis (forward curvature of the spine)
- Osteoporosis
- Cardiovascular abnormalities: Aortic insufficiency/aortitis, arrhythmias, angina, cardiomyopathy
- Respiratory abnormalities: Chest pain that affects breathing, restrictive disease, upper lobe fibrosis
- Jaw inflammation
- Cauda equina syndrome (rare)
- Patients with AS may also have psoriasis and/or inflammatory bowel disease
Extra-articular manifestations

Treatment
- Medications: Relieve pain and reduce inflammation
- Non-steroidal anti-inflammatory drugs (NSAIDs): Ibuprofen and naproxen
- Corticosteroids: i.v. methylprednisolone
- Disease-modifying anti-rheumatic drugs (DMARDs): Sulfasalazine
- TNF-α inhibitors: Infliximab, adalimumab, and etanercept
- Exercise: To reduce pain and stiffness
- Physical therapy: Improve comfort and spinal flexibility
- Surgery (rare): Repair significantly damaged joints or correct severe bends in the spine
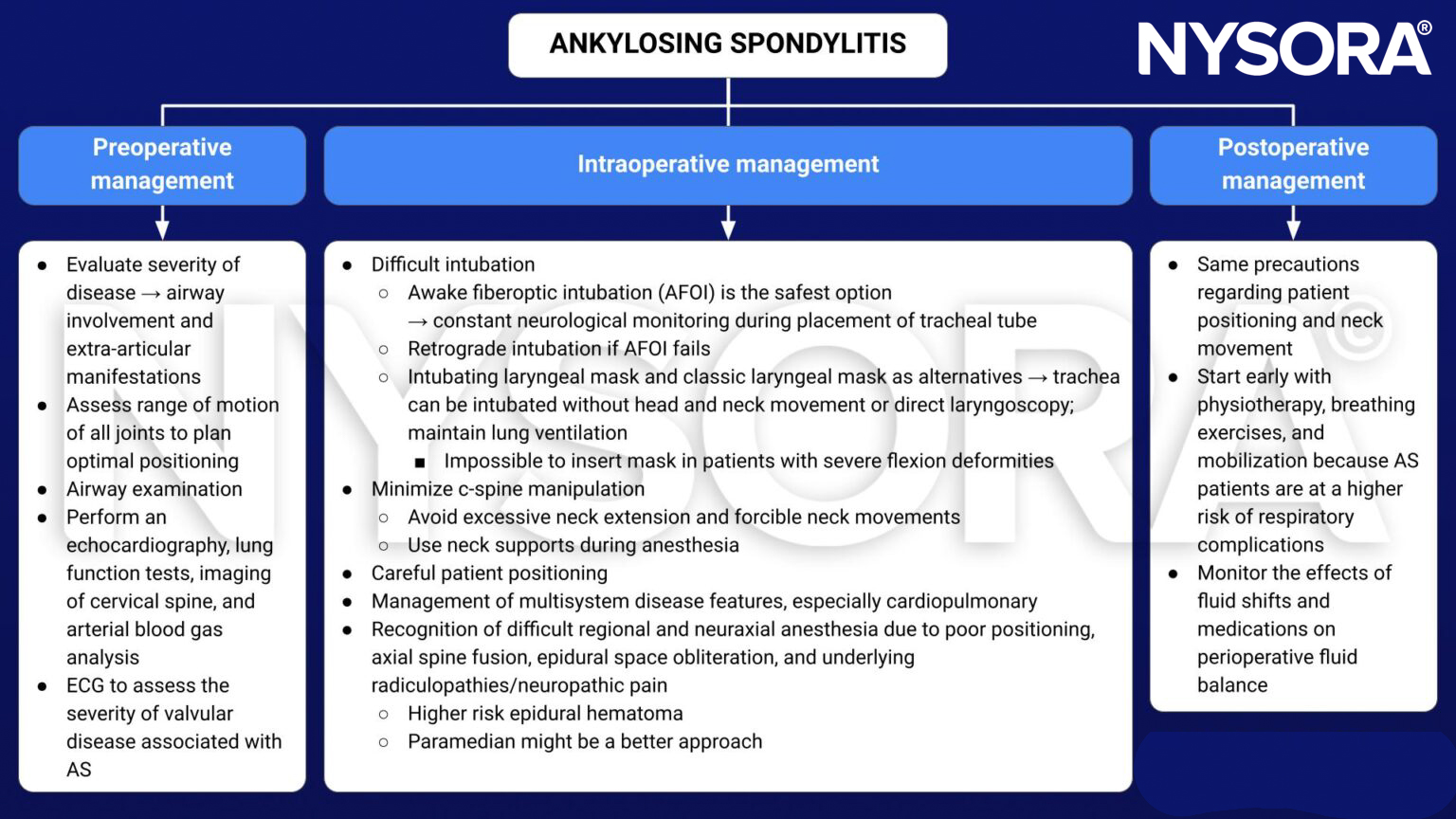
Management
Obstetrical anesthesia
- Complicated due to difficult airway and difficult neuraxial techniques → have multiple plans in place
- Consider paramedian approach and ultrasound guidance for neuraxial anesthesia
Keep in mind
- AS is a challenge for the anesthesiologist because the rigid, immobile, fragile spine makes intubation, general anesthesia, and neuraxial anesthesia difficult
- Awake fiberoptic intubation is the safest method of securing the airway in AS patients, but supraglottic airway devices such as laryngeal masks can also be used
- The use of alternative approaches, such as the paramedian approach or the use of ultrasound guidance, may improve success with neuraxial anesthesia in AS patients
Suggested reading
- Pahwa D, Chhabra A, Arora MK. Anaesthetic management of patients with ankylosing spondylitis. Trends in Anaesthesia and Critical Care. 2013;3(1):19-24.
- Woodward LJ, Kam PC. Ankylosing spondylitis: recent developments and anaesthetic implications. Anaesthesia. 2009;64(5):540-548.