Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
AboutIndications
Abdominal free fluid is often present with:
- Hepatic, renal, or cardiac failure (ascites)
- Inflammation or abdominal sepsis
- Hemorrhage
- Malignancy
Tips
- The exam for free intraperitoneal fluid is a ‘rule-in’ exam and is specifically focused on the detection of intra-abdominal fluid.
- The presence of small amounts of abdominal fluid may be normal, as during the periovulatory period in females.
Functional anatomy
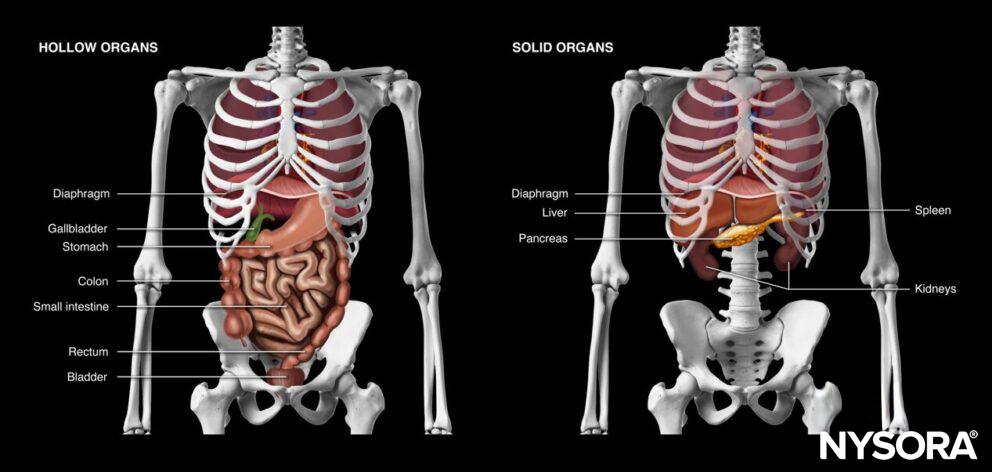
Hollow and solid abdominal organs.
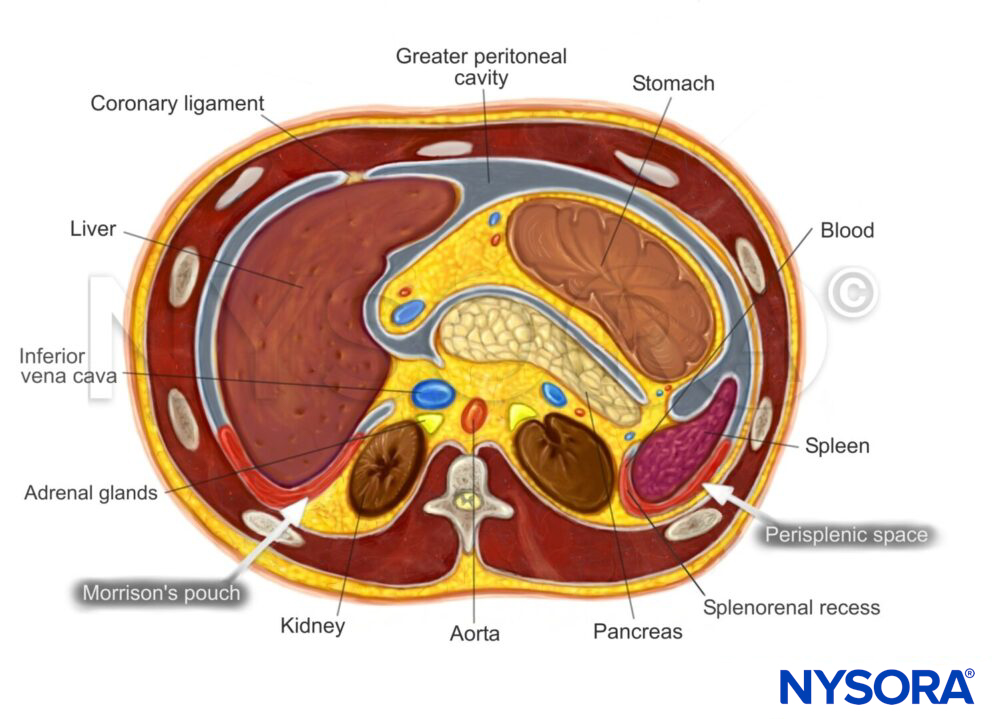
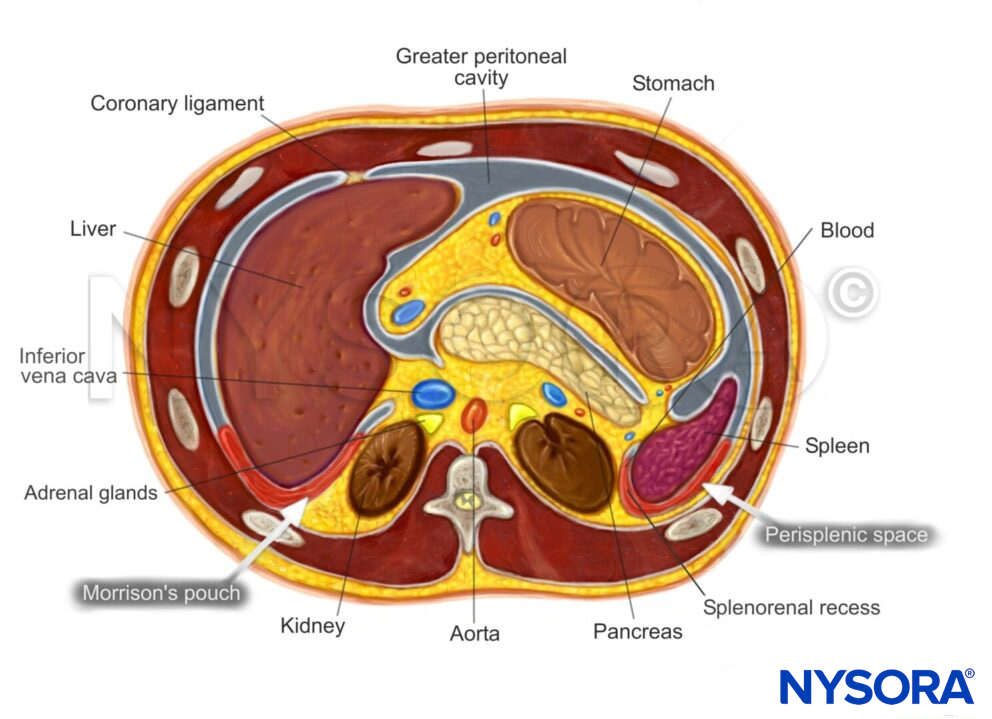
Intraperitoneal fluid tends to accumulate in the greater peritoneal cavity surrounding the abdominal organs. Due to gravity, the most likely anatomical sites of fluid collection are in the space between the liver and the kidney (Morrison’s pouch), the space surrounding the spleen (perisplenic space), or the rectovesical/rectouterine pouch.
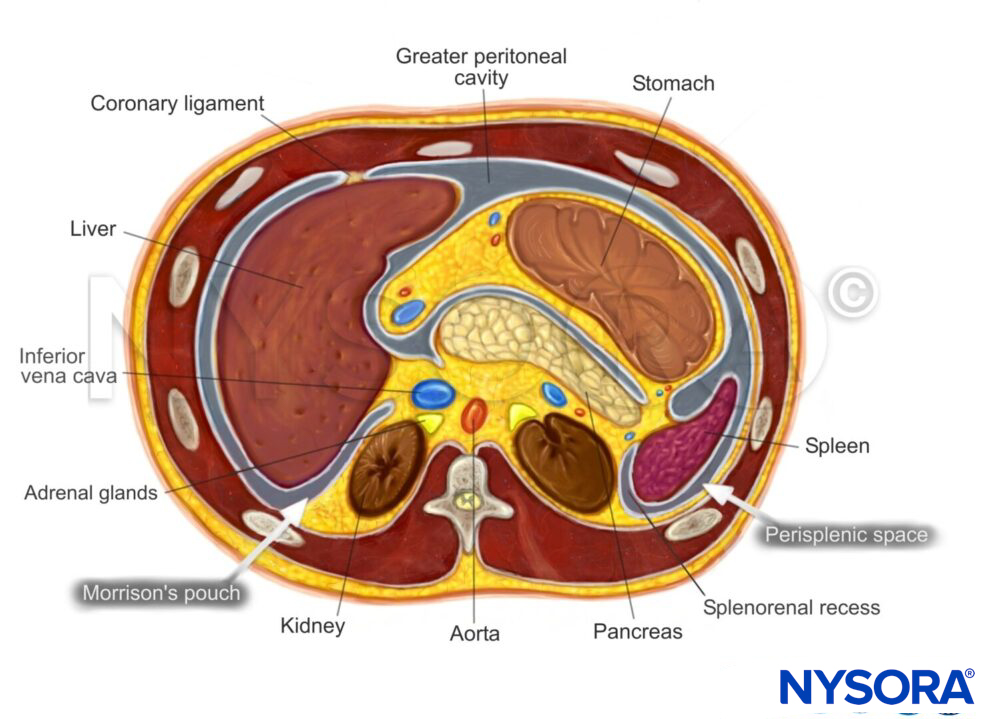
Transverse section through the upper abdomen.
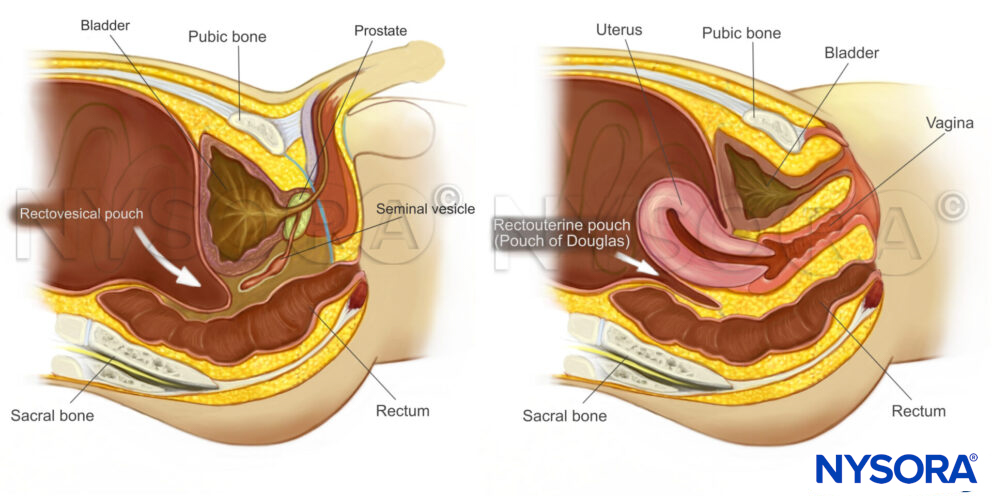
Sagittal section through the pelvis.
Ultrasound machine setup
- Transducer: Curvilinear (or phased array)
- Ultrasound preset: Abdominal
- Orientation: Index mark toward the right side of the patient or cranial
- Depth: 10-15 cm
Patient position
Position the patient supine and flat, with the arms abducted. If not flat, the fluid will shift and accumulate in the pelvis.

Patient position for free intraperitoneal fluid assessment.
Landmarks
- Costal margin: Ribs in the upper abdomen protect the upper abdominal organs but may limit the acoustic window to the liver, spleen and kidneys.
- Xiphoid process: The upper border of the abdomen.
- Linea alba: Midline of the abdomen that separates the rectus abdominis muscles and connects the xiphoid process with the pubic bone.
- Umbilicus: Virtually separates the abdomen into four quadrants
- Pubic bone: Bony structure and lower margin of the abdomen. The pelvis starts at the level of the pubic bone.
- Anterior superior iliac spine: Bony structure that forms the lateral border of the pelvis.
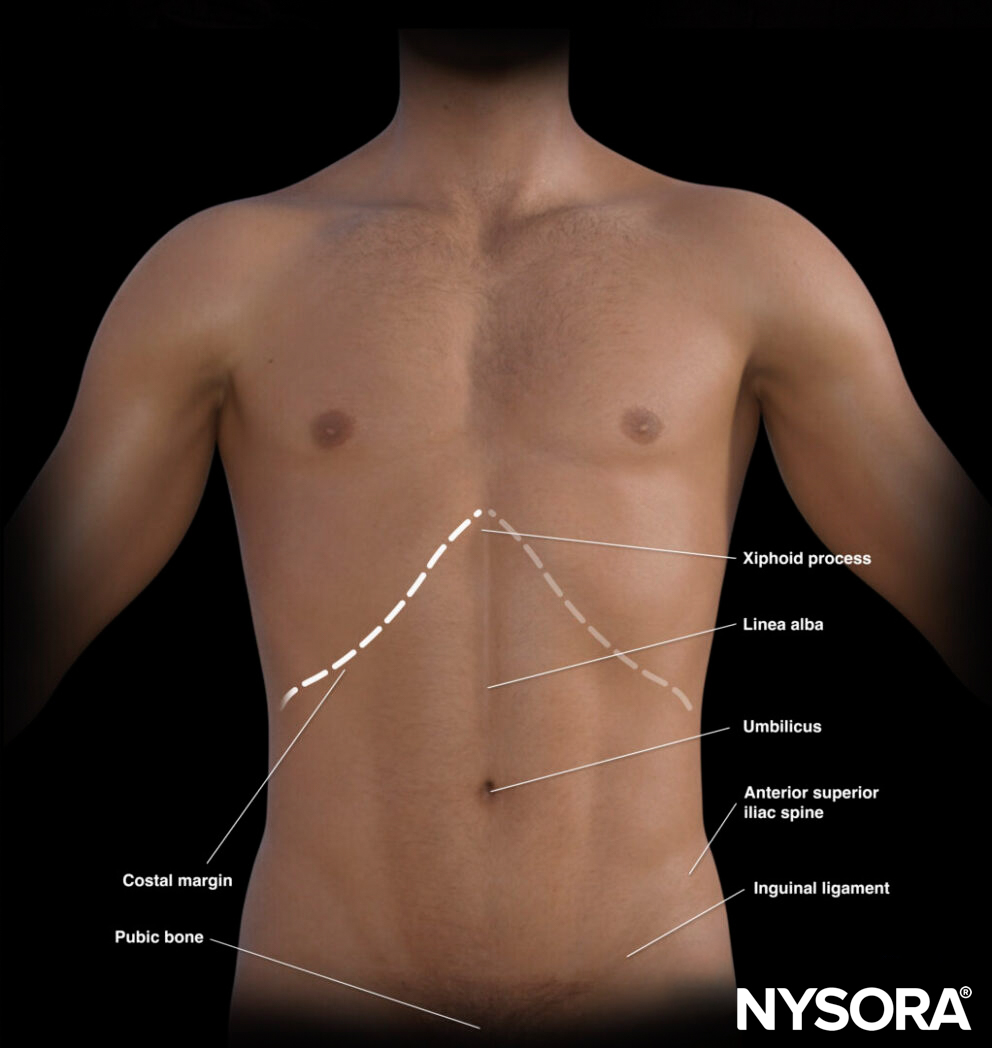
External landmarks of the abdomen.
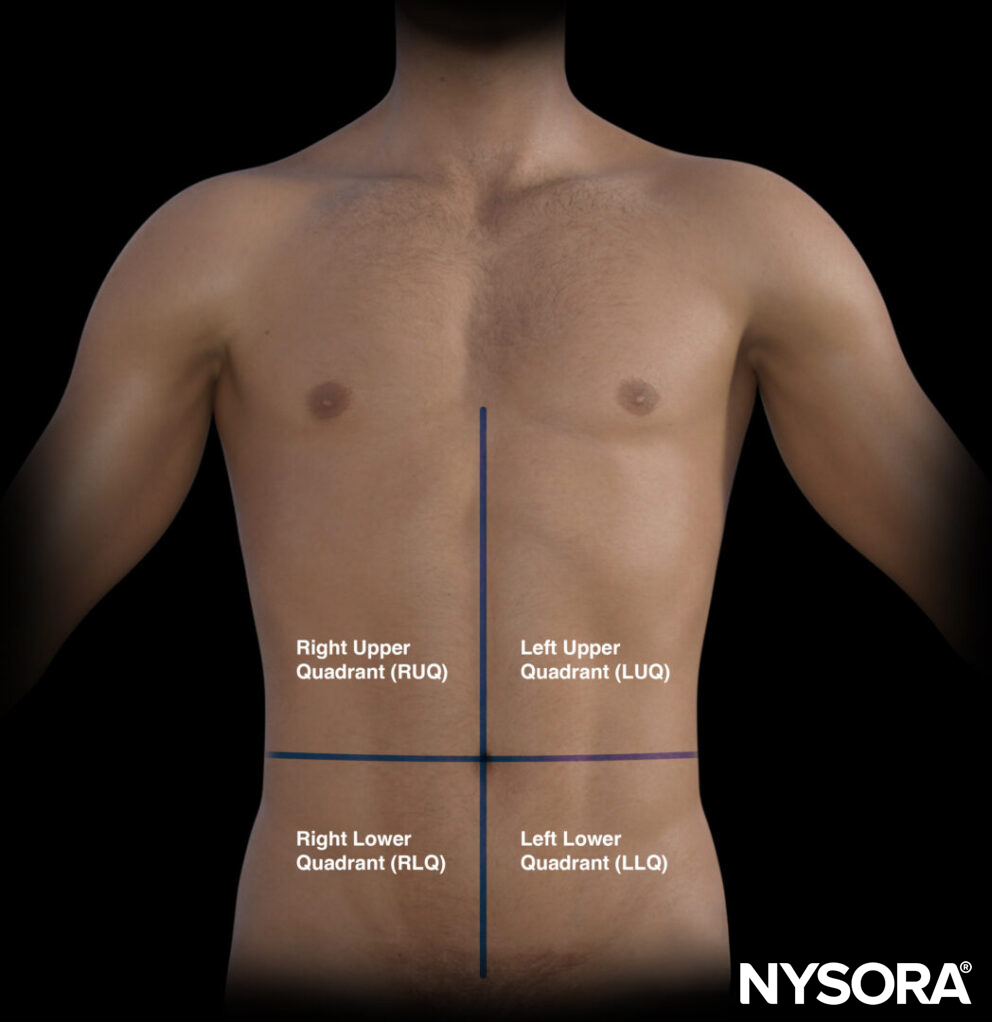
The umbilicus also divides the abdomen into four quadrants that surface-map key organs.
- Right upper quadrant (RUQ): Liver, gallbladder, kidney
- Left upper quadrant (LUQ): Stomach, spleen, kidney
- Pelvic/paracolic region (lower quadrants) (LLQ & RLQ): Colon, small intestines, rectum, bladder, male or female reproductive organs
Transducer position
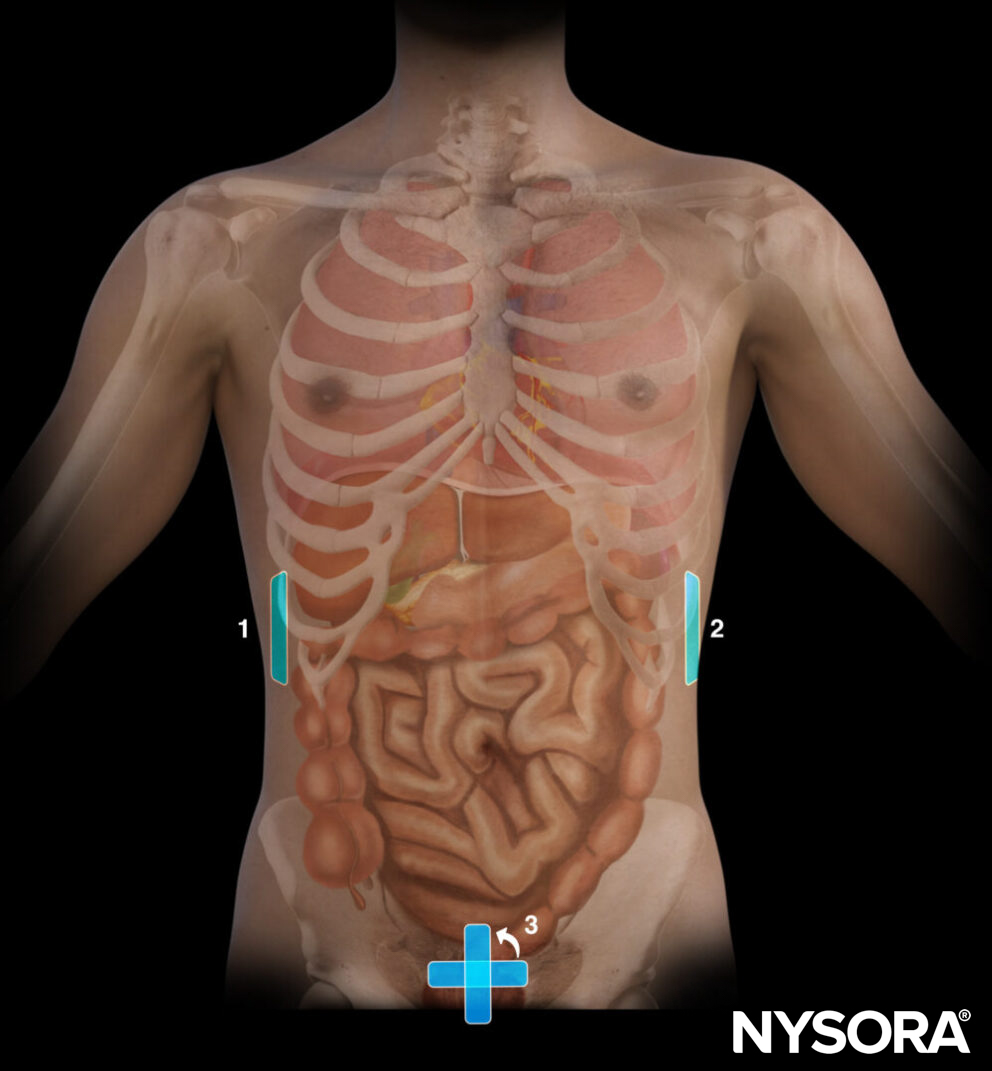
Different areas for transducer positioning for a free intraperitoneal fluid scan: 1, RUQ; 2, LUQ; 3, Suprapubic area.
A scan for free intraperitoneal fluid is performed in these three areas:
- The right upper quadrant (RUQ): Place the transducer between the mid- and the posterior axillary line at the level of the xiphoid process and start scanning caudally until you visualize the liver and the kidney
- The Left upper quadrant (LUQ): Place the transducer on the posterior axillary line at the level of the xiphoid process and start scanning caudally until you visualize the spleen and the kidney
- The suprapubic area for pelvic assessment: Place the transducer on the linea alba, just above the pubic bone.
Note
Fan and/or tilt the transducer in both directions in all scanning positions to increase the sensitivity for detecting free fluid.
Tips
- When scanning the upper abdominal quadrants, breathing makes imaging of the abdominal organs more challenging. The “curtain sign” is one of the examples of imaging difficulties even with normal respirations.
- Small rotational movements of the transducer can help to find an acoustic window between the ribs.
Scanning
Right upper quadrant (RUQ)
Detects free fluid in the right thorax and abdomen.
- Position the transducer between the mid- and posterior axillary lines at the level of the xiphoid process, with the orientation marker facing the patient’s head.
- Scan caudally until you visualize the liver and the kidney; fluid usually collects between the liver and the kidney, i.e., Morrison’s pouch.
Structures of interest: lung, diaphragm, liver, kidney, Morrison’s pouch (virtual space between liver and kidney)
Normal sonoanatomy:
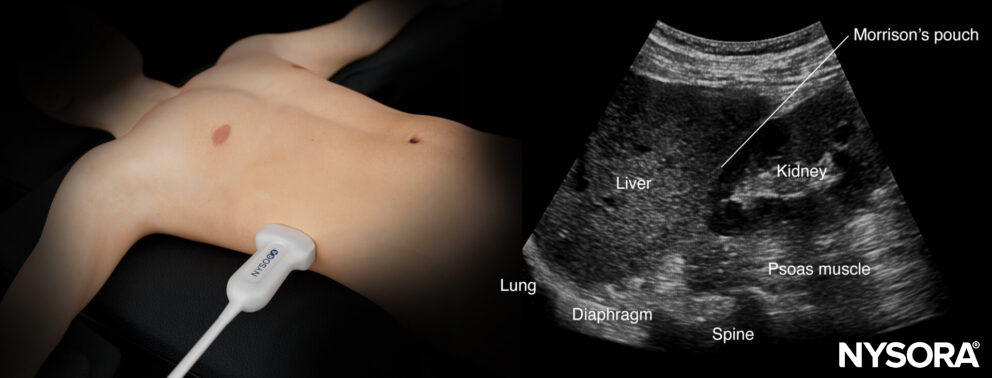
Ultrasound anatomy of the right upper quadrant and relevant anatomical structures.
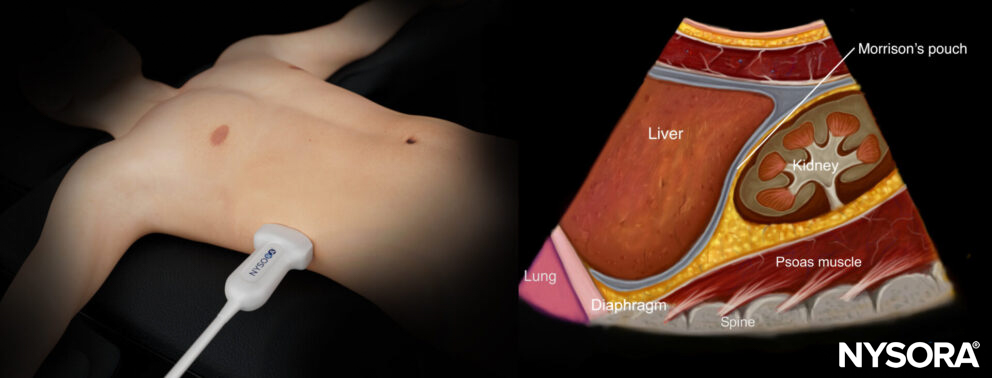
Reverse ultrasound anatomy of the right upper quadrant and relevant anatomical structures.
Free intraperitoneal fluid:
Free right intraperitoneal fluid collects between the liver and the kidney (Morrison’s pouch). If intrathoracic free fluid is present, it can be identified above the diaphragm.
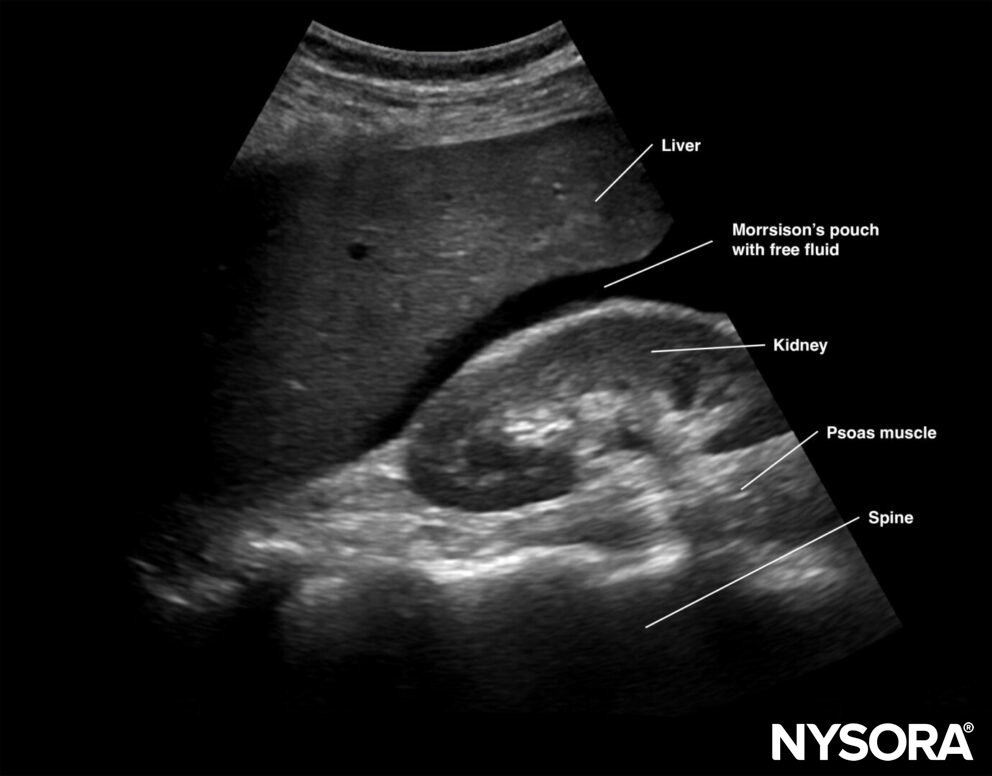
Free intraperitoneal fluid is often found between the liver and the kidney, i.e., Morrison’s pouch.
Tips
- Do not confuse the gallbladder with free fluid
- The liver can be used as an acoustic window toward other structures.
Left upper quadrant (LUQ)
This view allows free fluid assessment in the left thorax and abdomen.
- Position the transducer on the posterior axillary line in the LUQ with the orientation marker toward the head of the patient.
- Start scanning caudally until you visualize the spleen and the kidney.
- Structures of interest: lung, diaphragm, spleen, perisplenic space, kidney
Normal sonoanatomy:
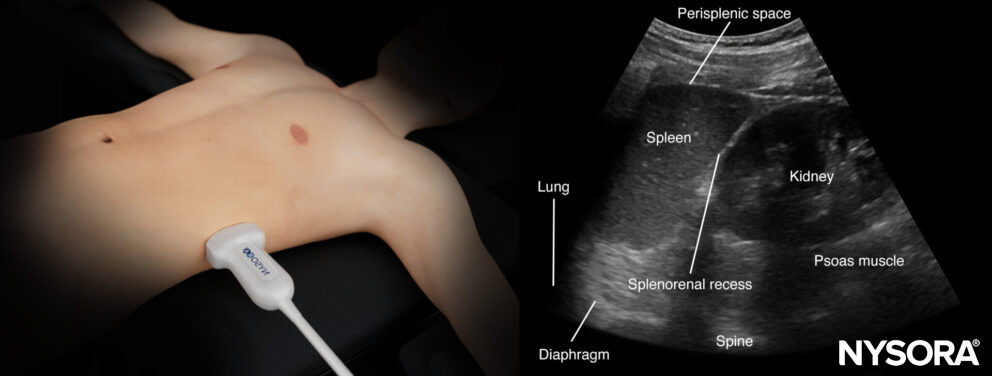
Ultrasound anatomy of the left upper quadrant and relevant anatomical structures.
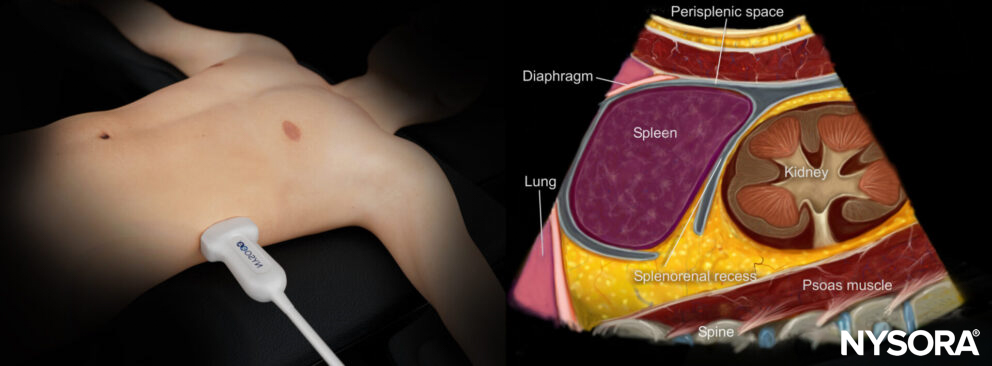
Reverse Ultrasound Ultrasound anatomy of the left upper quadrant and relevant anatomical structures.
Tips
- The position of the spleen is more cranial and posterior, which may make it harder to visualize
- Try directing the ultrasound beam more cranially to improve the image
Free intraperitoneal fluid:
Intraperitoneal fluid often collects between the spleen and the diaphragm (perisplenic space). Fluid may also accumulate in other locations, such as the splenorenal recess. If intrathoracic free fluid is present, it can be identified above the diaphragm.
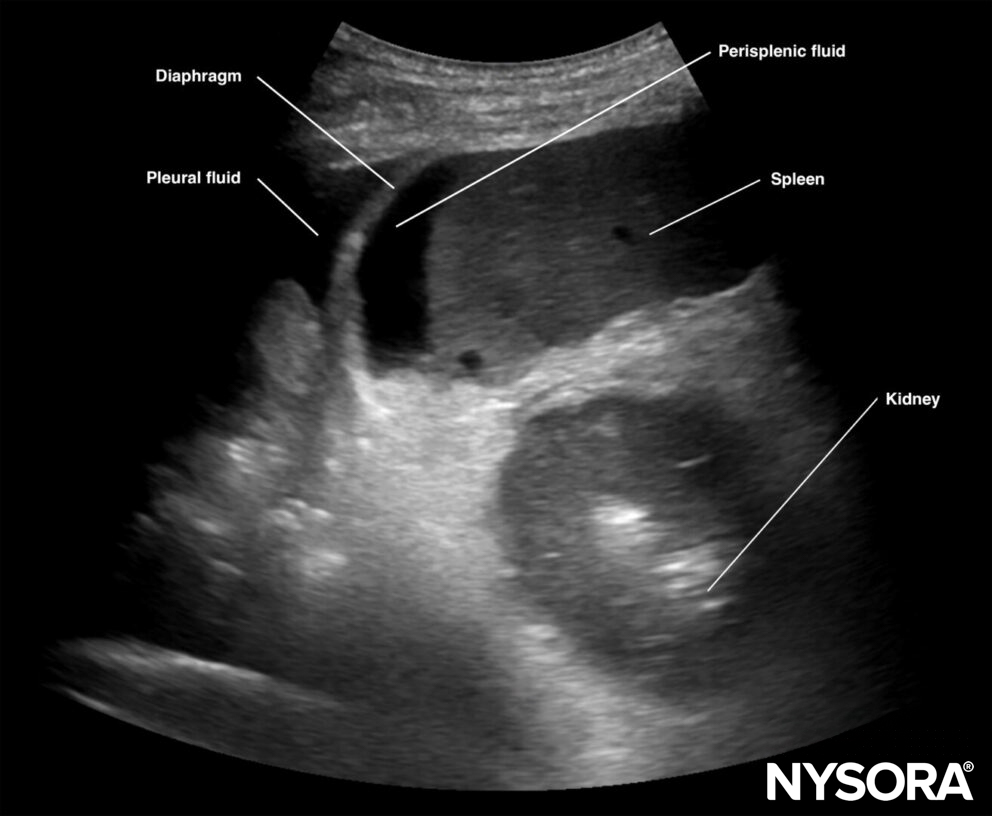
Free intraperitoneal fluid can be located in the perisplenic space.
Pelvis
This view assesses the presence of free fluid in the pelvis.
- Position the transducer just above the pubic bone in the midline between the umbilicus and the pubic bone.
- The bladder can be used as an internal anatomical landmark to scan the area behind and lateral to the bladder for free fluid (rectovesical pouch in men and the rectouterine pouch or pouch of Douglas in women).
Normal sonoanatomy:
- Longitudinal view (orientation marker toward the head)
Sonoanatomy of interest in females:
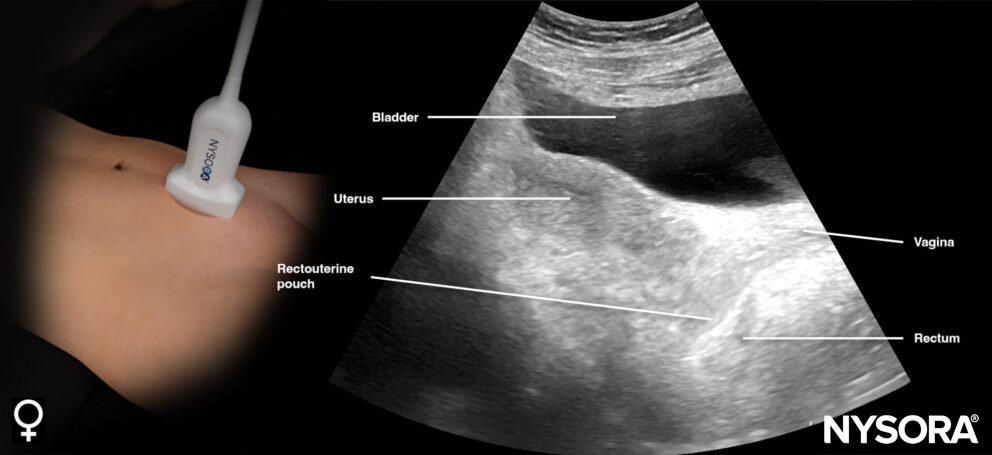
Transducer position and ultrasound anatomy of the female pelvis.
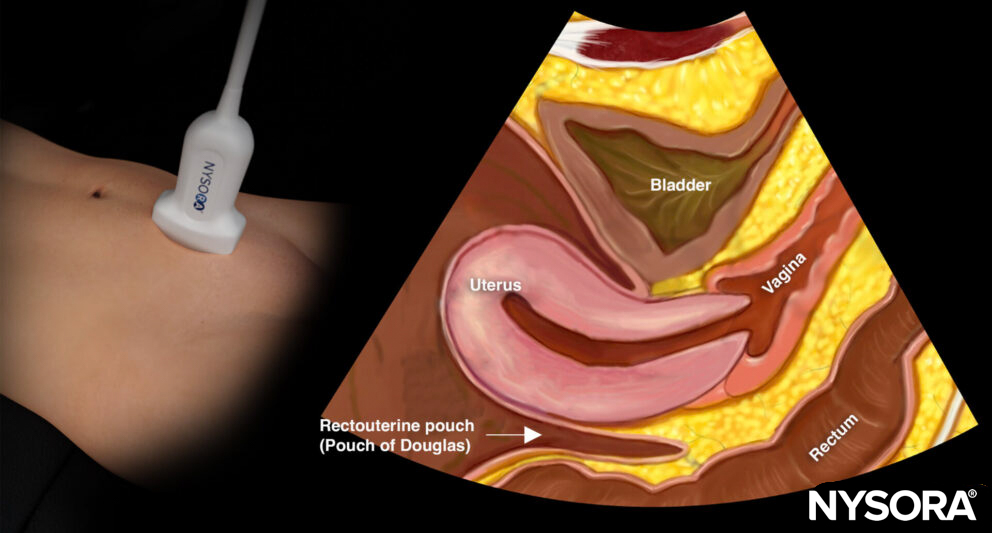
Transducer position and reverse ultrasound anatomy of the female pelvis.
Sonoanatomy of interest in males:
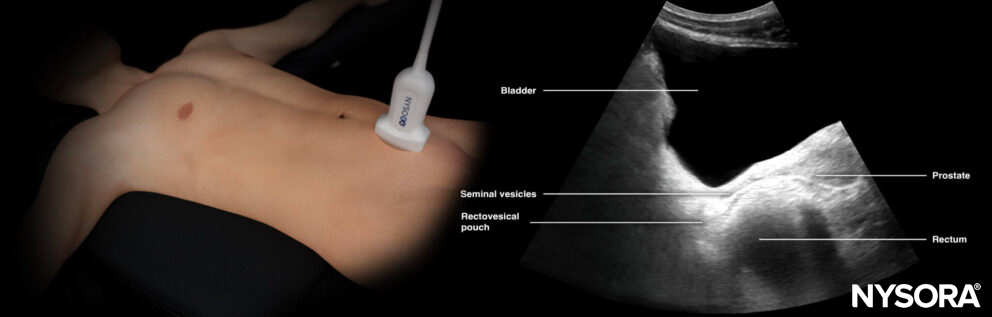
Transducer position and ultrasound anatomy of the male pelvis.
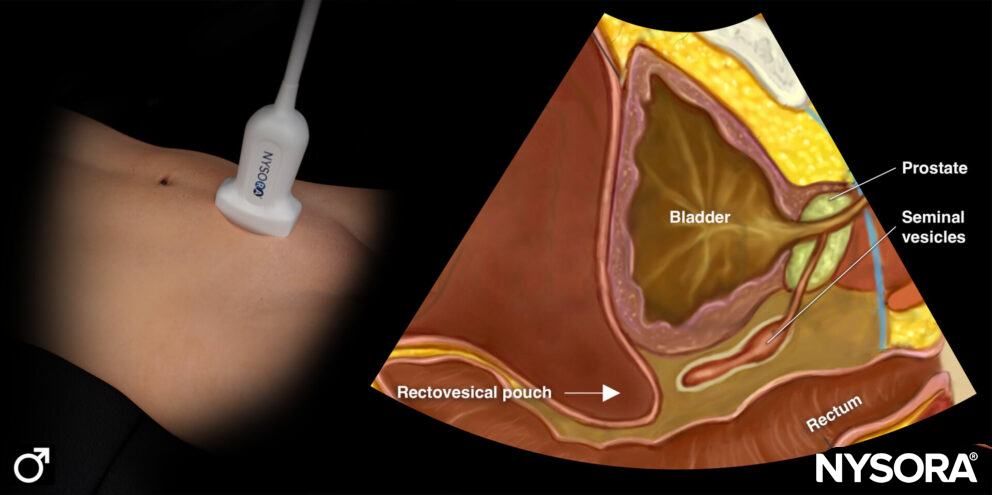
Transducer position and reverse ultrasound anatomy of the male pelvis.
- Transverse view (orientation marker toward the patient’s right)
Sonoanatomy of interest in females:
Transducer position and ultrasound anatomy of the female pelvis.
Transducer position and reverse ultrasound anatomy of the female pelvis.
Structures of interest in males:
Transducer position and ultrasound anatomy of the male pelvis.
Transducer position and reverse ultrasound anatomy of the male pelvis.
Free intraperitoneal fluid:
Pelvic free fluid collects behind the bladder or the area lateral to the bladder (rectovesical pouch in men and the rectouterine pouch or pouch of Douglas in women).
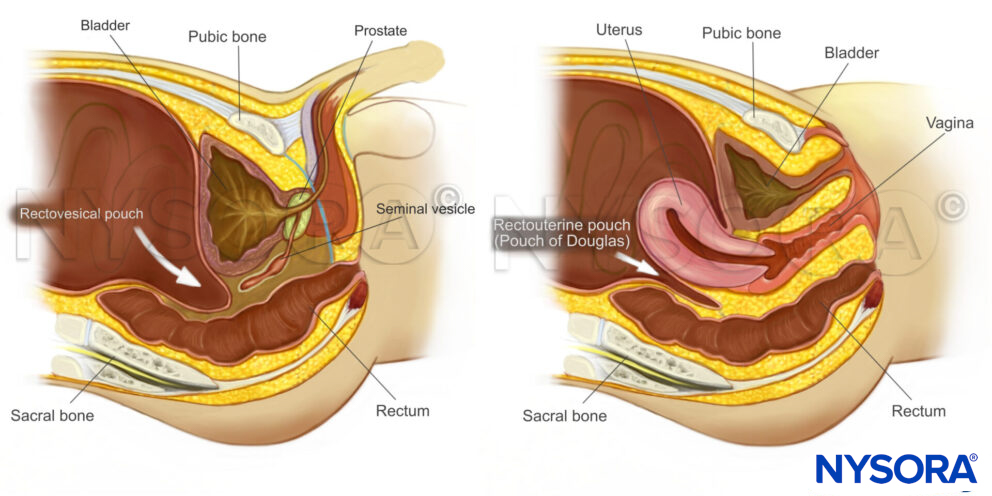
Sagittal section through the pelvis with free fluid in the rectovesical pouch in men and the rectouterine pouch (pouch of Douglas) in women.
Sonoanatomy of interest in females:
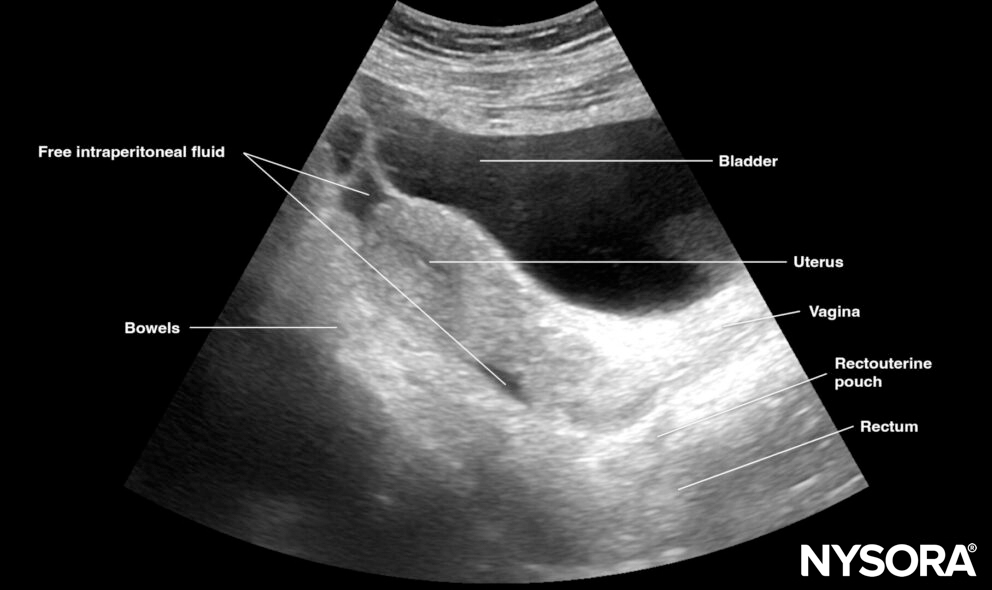
Longitudinal view of the female pelvis with free fluid in the rectouterine pouch.
Transverse view of the female pelvis with free fluid in the rectouterine pouch.
Sonoanatomy of interest in males:
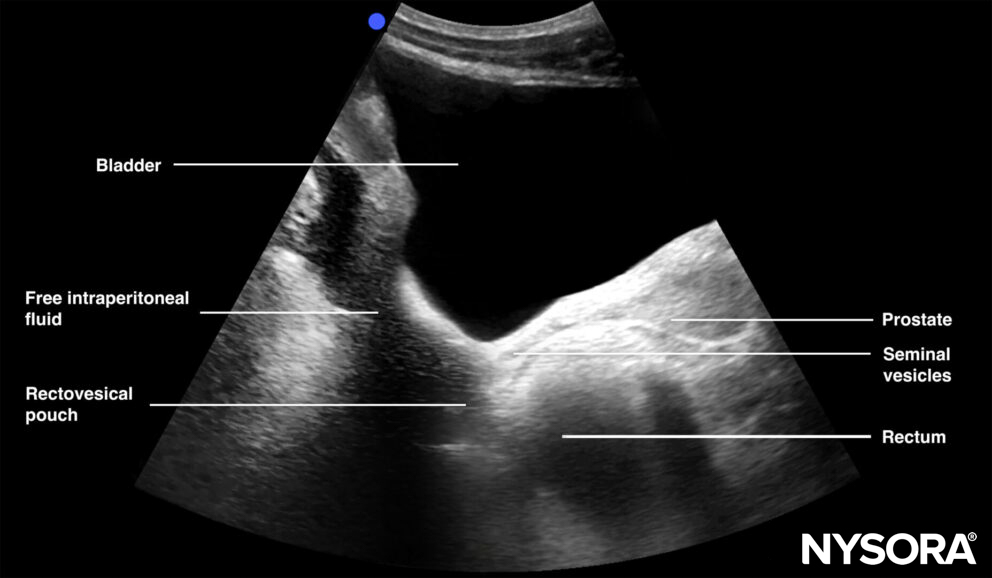
Longitudinal view of the male pelvis with free fluid in the rectovesical pouch after Foley catheter insertion.
Transverse view of the male pelvis with free fluid in the rectovesical pouch after Foley catheter insertion.
Tips
- In men, the seminal vesicles may be mistaken for free fluid. However, the vesicles are usually more triangular in shape and symmetrically spaced from the midline in the transverse view.
- Adjust the gain to atone for the acoustic enhancement of the bladder, which makes it more difficult to observe hypoechoic free fluid posterior to the bladder.
Clinical updates
Fornari and Lawson (Pediatric Emergency Care, 2021) review the role of FAST in pediatric blunt abdominal trauma (BAT) and conclude that, unlike in adults, FAST has variable sensitivity (20–80%) and cannot be used in isolation to rule out intra-abdominal injury (IAI) in children. Although a positive FAST in a hemodynamically unstable child may expedite operative management, up to one-third of children with IAI have no free intraperitoneal fluid, and FAST does not detect hollow viscus, retroperitoneal, or many solid organ injuries, limiting its standalone utility. The authors emphasize integrating FAST findings with clinical assessment and validated low-risk prediction rules to reduce unnecessary CT while avoiding missed injuries.
- Fornari MJ, Lawson SL. Pediatric Blunt Abdominal Trauma and Point-of-Care Ultrasound. Pediatr Emerg Care. 2021;37(12):624-629.