Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About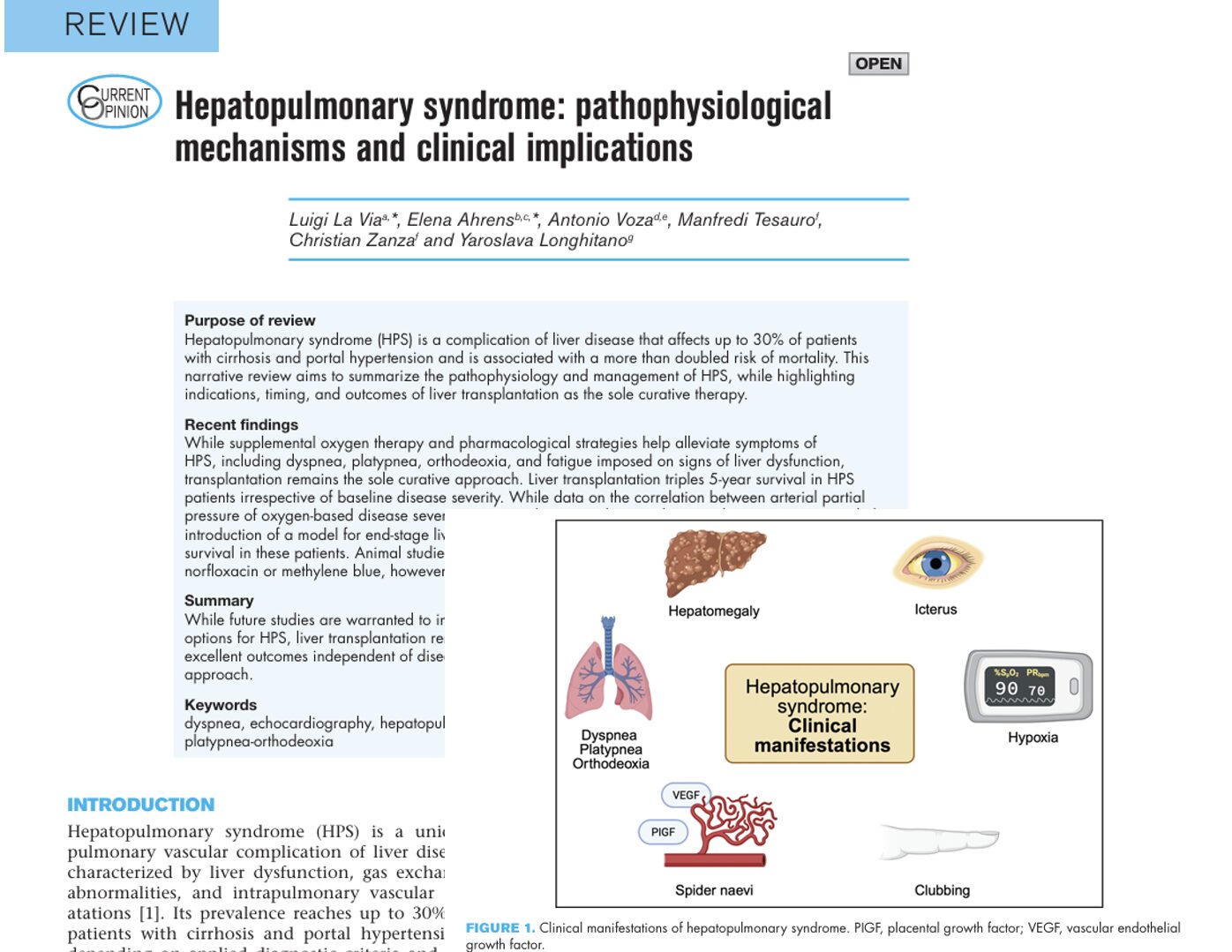




Hepatopulmonary syndrome (HPS) is a significant and often underdiagnosed complication of chronic liver disease. It affects approximately 30% of individuals with cirrhosis and portal hypertension and can more than double the risk of mortality. Despite its clinical importance, awareness remains limited. This post examines the underlying mechanisms, clinical features, diagnostic criteria, and the only curative treatment: liver transplantation.
What is hepatopulmonary syndrome?
HPS is a pulmonary vascular disorder uniquely linked to liver dysfunction. It is characterized by:
- Liver disease or portal hypertension
- Intrapulmonary vascular dilatations (IPVD)
- Abnormal arterial oxygenation
This triad leads to impaired gas exchange, often manifesting as chronic hypoxemia.
Pathophysiological mechanisms
-
Pulmonary vessel dilatation
- Capillary diameters can reach 100 µm in HPS (vs. 8–15 µm normally).
- Key mediators:
- Nitric oxide (NO): Overproduction due to liver dysfunction.
- Endothelin-1 (ET-1): Triggers NO synthesis despite being a vasoconstrictor.
- Carbon monoxide: Enhances NO-mediated vasodilation.
- Nitric oxide (NO): Overproduction due to liver dysfunction.
-
Angiogenesis
- Driven by elevated vascular endothelial growth factor (VEGF) and placental growth factor (PlGF).
- CD68(+) macrophages promote vessel proliferation.
-
Gas exchange abnormalities
- V/Q mismatch: Low ventilation-perfusion ratios.
- Intrapulmonary shunting: Arteriovenous connections bypass alveoli.
- Diffusion limitation: Thickened capillaries and high cardiac output reduce oxygen uptake.
Common symptoms and signs
Patients with HPS may present with:
- Dyspnea (most common; in ~80% of cases)
- Platypnea: Worsening breathlessness when upright
- Orthodeoxia: Drop in oxygen levels when sitting or standing
- Cyanosis and digital clubbing
- Fatigue (affects up to 85% of patients)
- Spider naevi
How is HPS diagnosed?
Key diagnostic triad:
- Chronic liver disease or portal hypertension
- Arterial hypoxemia (A-a gradient ≥ 15 mmHg, or ≥ 20 mmHg if over 65)
- Evidence of IPVD on imaging
Preferred diagnostic tools:
- Contrast-enhanced echocardiography: High sensitivity
- 99mTc-MAA lung perfusion scan: Detects shunts to extrapulmonary organs
HPS types:
- Type I: Precapillary dilatation (responds to oxygen)
- Type II: Direct AV shunts (oxygen therapy often ineffective)
Classification by severity
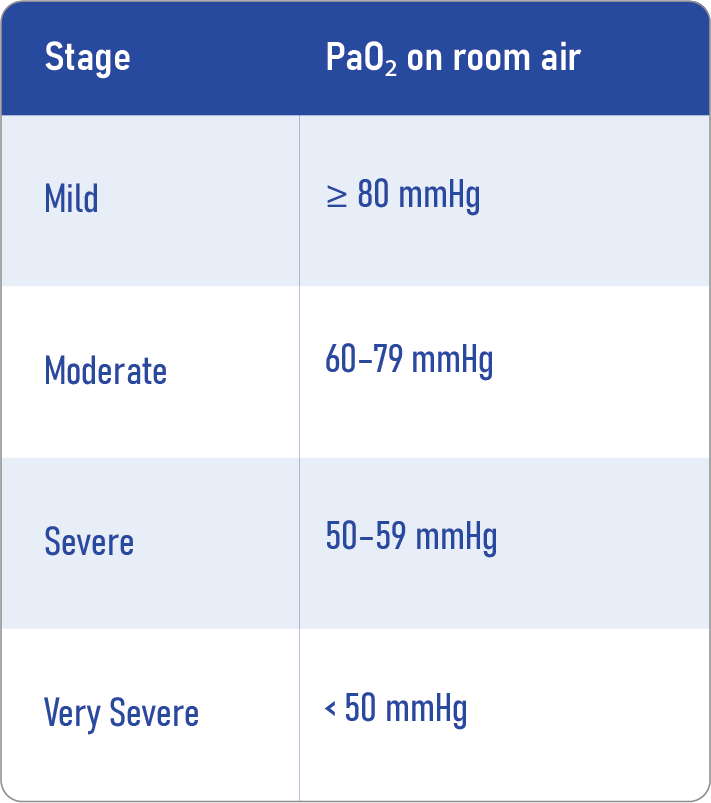
Severity affects transplant prioritization and prognosis.
Treatment options
Supportive care
- Supplemental oxygen: Indicated when PaO₂ < 90%; improves symptoms but not a cure.
Investigational pharmacological therapies
- Methylene blue: NO pathway inhibitor; improves gas exchange but is short-lived.
- Pentoxifylline: Limited efficacy in trials.
- Norfloxacin: Targets gut bacteria; promising in animals, inconclusive in humans.
- TNF-α inhibitors: Experimental phase.
Interventional options
- Transcatheter embolization: For localized AV malformations.
- TIPS (Transjugular intrahepatic portosystemic shunt): Variable results.
Liver transplantation: the only cure
Why it works
Transplantation addresses the root liver pathology, leading to reversal of vascular abnormalities and hypoxemia.
Indications
- Any HPS severity, especially PaO₂ <60 mmHg
- Rapid progression or symptomatic limitation
Timing considerations
- MELD exception points granted for PaO₂ <60 mmHg in the U.S.
- Caution with very severe hypoxemia (<50 mmHg), though recent studies show good outcomes.
Outcomes
- 5-year survival: 76% post-transplant vs. 23% without
- Symptom resolution: Usually within 6–12 months
- 1-year survival rate: ~90%
Steps for managing suspected HPS
- Identify symptoms (dyspnea, platypnea)
- Confirm liver disease
- Order arterial blood gas and contrast echocardiography
- Classify severity based on PaO₂
- Initiate oxygen therapy if indicated
- Evaluate for liver transplant
- Consider MELD exception points
- Monitor for disease progression and optimize pretransplant care
Conclusion
Hepatopulmonary syndrome is a complex but treatable condition when appropriately recognized. With early diagnosis and timely liver transplantation, most patients achieve full recovery and excellent long-term survival. Continued research is crucial for expanding treatment options and optimizing patient outcomes.
Reference: La Via L et al. Hepatopulmonary syndrome: pathophysiological mechanisms and clinical implications. Curr Opin Anaesthesiol. 2025;38:485-491.
For more information on rare complications, check out Anesthesia Updates on the NYSORA Anesthesia Assistant App.
Get access to step-by-step management algorithms, the latest research, and peer-reviewed insights—all in one place. Download the app today and experience the future of anesthesia education and decision-making.